Immunity acquired from a vaccine, also known as vaccine-induced immunity, is a critical aspect of public health that involves training the body’s immune system to recognize and combat specific pathogens, such as viruses or bacteria, without causing the disease itself. Vaccines typically contain a weakened, inactivated, or fragment of the pathogen, which prompts the immune system to produce antibodies and memory cells. This process prepares the body to mount a rapid and effective response if exposed to the actual pathogen in the future, significantly reducing the risk of infection or severe illness. Unlike natural immunity, which is gained after recovering from an infection and can vary in strength and duration, vaccine-induced immunity is a controlled and safer method of protection, often providing long-lasting defense against diseases and contributing to herd immunity when widespread vaccination is achieved.
| Characteristics | Values |
|---|---|
| Type of Immunity | Active immunity (body produces its own antibodies in response to vaccine) |
| Duration | Varies by vaccine; can be lifelong (e.g., measles) or require boosters |
| Mechanism | Stimulates the immune system to recognize and combat specific pathogens |
| Specificity | Targeted to specific pathogens or diseases (e.g., COVID-19, influenza) |
| Onset Time | Typically takes 1-2 weeks after vaccination for immunity to develop |
| Natural vs. Artificial | Artificial (induced by vaccination, not natural infection) |
| Memory Response | Creates immunological memory for faster response to future exposures |
| Herd Immunity Contribution | Reduces disease spread by increasing population immunity |
| Side Effects | Generally mild (e.g., soreness, fever) compared to natural infection |
| Examples | MMR (Measles, Mumps, Rubella), COVID-19 vaccines, Flu vaccines |
| Effectiveness | High but varies by vaccine and individual immune response |
| Booster Requirements | Some vaccines require periodic boosters to maintain immunity |
| Cross-Protection | Limited; vaccines are typically pathogen-specific |
| Impact on Public Health | Reduces morbidity, mortality, and disease outbreaks |
Explore related products






What You'll Learn
- Vaccine-induced active immunity: Vaccines expose the body to antigens, triggering immune response and memory cell production
- Passive immunity from vaccines: Some vaccines provide immediate, short-term protection via antibodies, not immune memory
- Herd immunity benefits: Vaccination reduces disease spread, protecting vulnerable populations who cannot be vaccinated
- Immune memory formation: Vaccines train the immune system to recognize and respond faster to future infections
- Vaccine efficacy factors: Effectiveness depends on vaccine type, dosage, individual health, and pathogen evolution
![]()
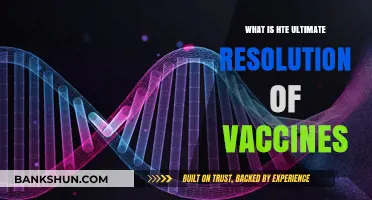
Vaccine-induced active immunity: Vaccines expose the body to antigens, triggering immune response and memory cell production
Vaccines are not just shots; they are sophisticated tools that teach the immune system to recognize and combat pathogens. At the heart of this process is vaccine-induced active immunity, a mechanism that mimics natural infection without the associated risks. When a vaccine is administered, it introduces antigens—harmless components of a pathogen—into the body. These antigens act as decoys, triggering an immune response without causing disease. For instance, the measles vaccine contains weakened measles viruses that prompt the immune system to produce antibodies and memory cells, preparing the body for future encounters with the actual virus.
Consider the steps involved in this process: First, the vaccine is delivered, often via intramuscular injection, such as the 0.5 mL dose of the MMR (measles, mumps, rubella) vaccine recommended for children aged 12–15 months. Next, antigen-presenting cells (APCs) engulf the antigens and transport them to lymph nodes, where they activate T cells and B cells. B cells differentiate into plasma cells, which secrete antibodies specific to the antigen. Simultaneously, memory B and T cells are generated, ensuring a rapid and robust response if the pathogen is encountered again. This orchestrated sequence is why vaccinated individuals often experience milder symptoms or no illness at all upon exposure to the real pathogen.
A comparative analysis highlights the efficiency of vaccine-induced immunity versus natural infection. While natural infection can lead to severe complications—such as pneumonia from measles or neurological damage from polio—vaccines provide a safer alternative. For example, the polio vaccine has nearly eradicated the disease globally, with cases dropping by over 99% since 1988. Unlike natural infection, vaccines are standardized, ensuring consistent antigen exposure and immune activation. This controlled approach minimizes risks while maximizing protection, making vaccines a cornerstone of public health.
Practical tips for optimizing vaccine-induced immunity include adhering to recommended schedules, as spacing doses appropriately (e.g., the two-dose regimen for the HPV vaccine, administered 6–12 months apart) allows for robust memory cell formation. Additionally, maintaining a healthy lifestyle—adequate sleep, balanced nutrition, and regular exercise—supports immune function. For parents, keeping a vaccination record ensures timely administration and reduces the risk of missed doses. Finally, staying informed about vaccine updates and booster recommendations is crucial, as immunity can wane over time, as seen with the tetanus booster advised every 10 years.
In conclusion, vaccine-induced active immunity is a testament to the immune system’s adaptability and the ingenuity of medical science. By exposing the body to antigens in a controlled manner, vaccines not only prevent disease but also foster long-term immune memory. This mechanism has saved millions of lives, from eradicating smallpox to controlling diseases like hepatitis B. Understanding this process empowers individuals to make informed decisions, ensuring they and their communities remain protected against preventable illnesses.
California Vaccine Registration Guide: Simple Steps to Schedule Your Shot
You may want to see also
Explore related products






![]()
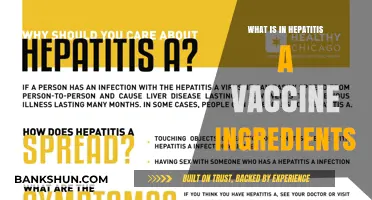
Passive immunity from vaccines: Some vaccines provide immediate, short-term protection via antibodies, not immune memory
Vaccines are typically celebrated for their ability to confer long-term immunity by training the immune system to recognize and combat pathogens. However, not all vaccines operate this way. Some, like the rabies vaccine, provide passive immunity, a short-term defense mechanism that bypasses immune memory altogether. Instead of stimulating the body to produce its own antibodies, these vaccines directly deliver pre-formed antibodies or antibody-producing components, offering immediate protection that wanes over weeks to months. This approach is particularly critical in emergency situations, such as post-exposure prophylaxis, where rapid defense is essential.
Consider the rabies vaccine, a prime example of passive immunity in action. When administered after a potential exposure—such as a bite from an infected animal—it includes both an active component (to stimulate immune memory) and a passive component (rabies immunoglobulin). The immunoglobulin, derived from human or equine sources, provides instant antibodies to neutralize the virus before it can establish infection. This dual strategy is lifesaving, as rabies is nearly 100% fatal once symptoms appear. However, the passive protection lasts only 2–3 weeks, underscoring its temporary nature.
Passive immunity is not limited to rabies. For instance, the tetanus immunoglobulin (TIG) is administered alongside the tetanus vaccine in cases of deep or dirty wounds to provide immediate protection against the toxin. Similarly, the RSV (respiratory syncytial virus) monoclonal antibody injection, given to high-risk infants, offers passive immunity for the duration of the RSV season. These interventions are particularly valuable for vulnerable populations, such as the immunocompromised or those with incomplete vaccination histories, who cannot mount a robust immune response.
While passive immunity is a powerful tool, it comes with limitations. Unlike active immunity, which can last years or a lifetime, passive protection is fleeting. For example, the half-life of administered antibodies is typically 21–28 days, meaning their effectiveness diminishes rapidly. Additionally, repeated doses can lead to hypersensitivity reactions, particularly with non-human derived antibodies. Therefore, passive immunity is reserved for specific scenarios where immediate protection is non-negotiable, not as a substitute for long-term immune memory.
In practice, understanding the role of passive immunity can guide better decision-making. For travelers to rabies-endemic regions, knowing that post-exposure prophylaxis includes both active and passive components can emphasize the urgency of seeking treatment. For parents of premature infants, awareness of RSV monoclonal antibody injections can help them advocate for timely administration. Clinicians, too, must weigh the benefits of immediate protection against the transient nature of passive immunity, ensuring it complements, rather than replaces, active vaccination strategies. In short, passive immunity is a vital, if temporary, shield in the arsenal of vaccine-mediated defense.
Contact Synchrony Bank Amazon: Address and Communication Guide
You may want to see also
Explore related products






![]()
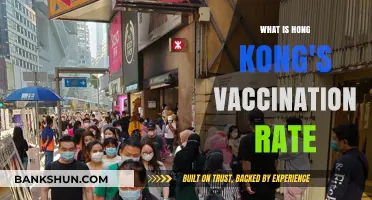
Herd immunity benefits: Vaccination reduces disease spread, protecting vulnerable populations who cannot be vaccinated
Vaccination doesn’t just shield the individual; it erects a firewall against disease spread, a phenomenon known as herd immunity. When a critical mass of a population is immunized—typically 70-90%, depending on the disease’s contagiousness—the pathogen struggles to find susceptible hosts, effectively halting outbreaks. Measles, for instance, requires 95% vaccination coverage to disrupt transmission due to its high infectivity (R0 of 12-18). Achieving this threshold doesn’t merely reduce case numbers; it protects those who cannot be vaccinated due to medical reasons, such as infants under 12 months (too young for MMR vaccines) or immunocompromised individuals (e.g., chemotherapy patients). This collective defense mechanism transforms vaccination from a personal choice into a communal responsibility.
Consider the practical steps to maximize herd immunity. For diseases like pertussis (whooping cough), where immunity wanes over time, adolescents and adults require booster doses (Tdap) to maintain protection. Pregnant women are advised to receive Tdap during the third trimester, passing antibodies to newborns who cannot be vaccinated until 2 months old. Similarly, annual flu vaccination campaigns prioritize healthcare workers, elderly populations, and those with chronic conditions, as these groups are both high-risk and potential vectors for spread. Schools and workplaces can enforce vaccination policies (e.g., requiring MMR proof for enrollment) to close immunity gaps, though exemptions must be carefully managed to avoid excluding vulnerable individuals unnecessarily.
Critics often argue that herd immunity renders individual vaccination optional, but this logic crumbles under scrutiny. Take polio: in the 1980s, global cases plummeted from 350,000 annually to fewer than 100 by 2020 due to vaccination campaigns, yet even small pockets of unvaccinated populations (e.g., in Afghanistan and Pakistan) allowed the virus to persist. Similarly, the 2019 measles outbreak in the U.S., concentrated in under-vaccinated communities, demonstrated how localized immunity gaps can reignite eradicated diseases. Herd immunity is not a passive byproduct of vaccination but an actively maintained state, requiring vigilance and equitable access to vaccines worldwide.
The ethical imperative of herd immunity lies in its protection of the most vulnerable. For example, children with leukemia, whose immune systems are suppressed by treatment, rely on community immunity to avoid exposure to preventable diseases. Similarly, organ transplant recipients, who take immunosuppressants to prevent rejection, cannot mount an immune response to vaccines, making herd immunity their sole shield. Public health strategies must therefore balance individual rights with collective obligations, ensuring that vaccine hesitancy or inaccessibility does not undermine this fragile safety net. Practical measures, such as mobile vaccination clinics in underserved areas or multilingual educational campaigns, can bridge these gaps and fortify herd immunity for all.
Sasha Banks' Championship Reign: A Timeline of Her Title Success
You may want to see also
Explore related products






![]()
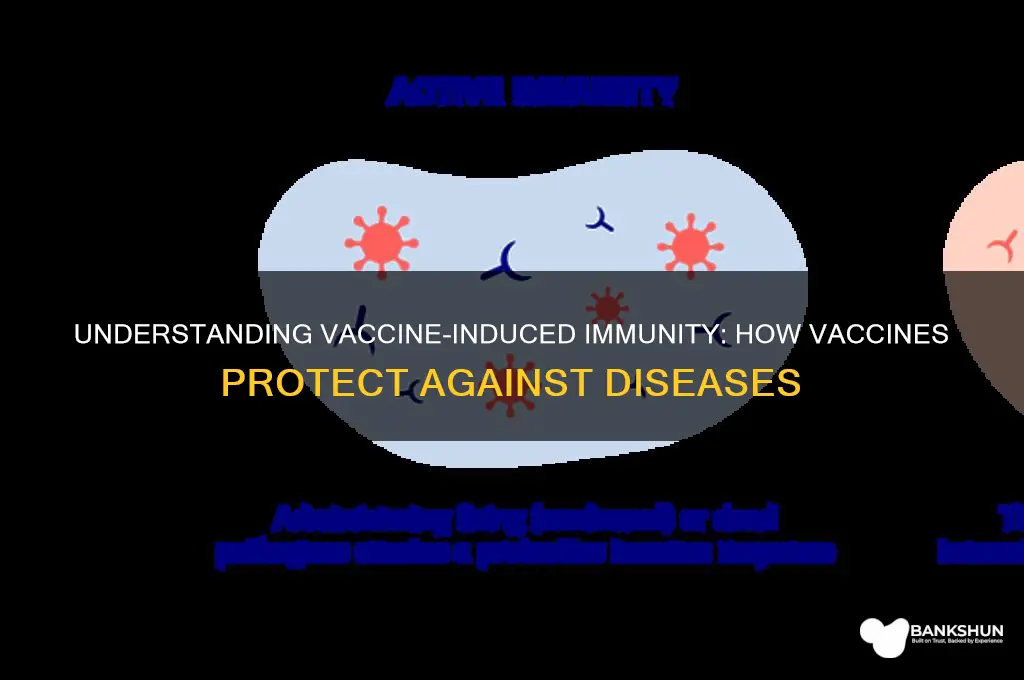
Immune memory formation: Vaccines train the immune system to recognize and respond faster to future infections
Vaccines are not just preventive measures; they are educators, teaching the immune system to recognize and combat pathogens with precision and speed. At the heart of this process is immune memory formation, a biological mechanism that ensures the body’s defense system is primed for future encounters with the same pathogen. When a vaccine introduces a harmless piece of a virus or bacterium (or a weakened/inactivated form of it), the immune system responds by producing antibodies and activating specialized cells like T cells and B cells. While this initial response mimics a natural infection, it is far safer because the vaccine does not cause disease. Critically, some of these activated cells transform into memory cells, which persist long after the vaccine antigen is cleared. These memory cells are the immune system’s archive, storing the blueprint of the pathogen for rapid recall.
Consider the influenza vaccine, administered annually to millions worldwide. Each dose contains inactivated virus particles tailored to the year’s dominant strains. Upon injection, typically 0.5 mL for adults and 0.25 mL for children aged 6–35 months, the immune system mounts a response, generating antibodies and memory cells. If the vaccinated individual later encounters the live virus, these memory cells leap into action, producing antibodies up to 100 times faster than during the initial exposure. This accelerated response neutralizes the virus before it can cause severe illness, often reducing symptoms to mild or none at all. Without this immune memory, the body would treat each infection as a first encounter, leaving it vulnerable during the days-long process of antibody production.
The formation of immune memory is not instantaneous; it requires time and, often, multiple doses. For instance, the measles, mumps, and rubella (MMR) vaccine is given in two doses, typically at 12–15 months and 4–6 years of age. The first dose primes the immune system, creating an initial wave of memory cells. The second dose acts as a booster, significantly increasing the number and potency of these cells, ensuring long-lasting immunity. This dosing strategy is critical because memory cells wane over time, and their numbers directly correlate with the strength of future responses. In contrast, natural infections can also create immune memory, but they carry the risk of severe complications, making vaccines the safer alternative for memory formation.
To maximize the benefits of immune memory, adherence to recommended vaccine schedules is essential. For example, the COVID-19 mRNA vaccines, such as Pfizer-BioNTech and Moderna, require two doses spaced 3–4 weeks apart for optimal memory cell development. Studies show that this regimen reduces symptomatic infection rates by over 90% and hospitalization by 95%. However, real-world data also highlights the importance of timing; delaying the second dose beyond the recommended interval diminishes the memory response, leaving individuals partially protected. Similarly, age-specific considerations matter: older adults, whose immune systems naturally weaken with age, may require additional doses or adjuvanted vaccines to achieve robust memory formation.
Practical tips can enhance the immune memory process. Maintaining a healthy lifestyle—adequate sleep, balanced nutrition, and regular exercise—supports overall immune function, potentially improving vaccine efficacy. For parents, keeping a detailed record of their child’s vaccinations ensures timely administration of booster doses, critical for memory cell reinforcement. Lastly, staying informed about updated vaccine formulations, such as seasonal flu shots or variant-specific COVID-19 boosters, allows individuals to adapt their immunity to evolving pathogens. By understanding and supporting immune memory formation, vaccines transform the body into a well-prepared fortress, ready to defend against future threats with speed and efficiency.
Understanding the Role of a Personal Banker in the UK
You may want to see also
Explore related products






![]()
Vaccine efficacy factors: Effectiveness depends on vaccine type, dosage, individual health, and pathogen evolution
Vaccines are not one-size-fits-all solutions. Their effectiveness hinges on a delicate interplay of factors, each influencing how well our bodies mount a protective immune response. Let's dissect these critical variables: vaccine type, dosage, individual health, and the ever-evolving nature of pathogens.
Imagine a toolbox – different tools for different jobs. Similarly, vaccines employ diverse strategies to train our immune system. Live-attenuated vaccines, like the measles-mumps-rubella (MMR) shot, use weakened viruses to trigger a robust immune memory. Inactivated vaccines, such as the injectable polio vaccine, present killed pathogens for immune recognition. Subunit vaccines, like the hepatitis B vaccine, deliver specific protein fragments, while mRNA vaccines, a newer technology exemplified by Pfizer-BioNTech's COVID-19 vaccine, provide genetic instructions for our cells to produce viral proteins, prompting an immune response. Each type has its strengths and limitations, impacting efficacy.
Dosage isn't just about quantity; it's about precision. Too little might fail to stimulate a sufficient immune response, while too much could lead to unnecessary side effects. The optimal dose varies depending on the vaccine type, the pathogen targeted, and the recipient's age. For instance, infants receive smaller doses of certain vaccines compared to adults due to their developing immune systems. Booster shots, administered months or years after the initial series, reinforce immune memory, ensuring continued protection.
Admittedly, our bodies aren't identical immune fortresses. Age, underlying health conditions, and lifestyle factors significantly influence vaccine efficacy. Older adults, for example, may experience a decline in immune function, making them more susceptible to infections and potentially less responsive to vaccination. Individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, may require specialized vaccination schedules or alternative vaccine types.
Pathogens are cunning adversaries, constantly evolving to evade our defenses. This evolutionary arms race poses a significant challenge to vaccine efficacy. Influenza viruses, notorious for their rapid mutation, necessitate annual vaccine updates to match the circulating strains. Similarly, the emergence of new SARS-CoV-2 variants has prompted the development of updated COVID-19 booster shots. This ongoing battle underscores the need for continuous surveillance, research, and vaccine adaptation to stay ahead of these ever-changing threats.
Understanding these efficacy factors empowers us to make informed decisions about vaccination. It highlights the importance of personalized approaches, considering individual health status and the specific vaccine characteristics. Moreover, it emphasizes the need for ongoing research and innovation to develop more effective vaccines and strategies to combat the relentless evolution of pathogens. By acknowledging these complexities, we can appreciate the remarkable achievements of vaccination while recognizing the ongoing efforts required to maintain and improve its protective power.
Syncing Synchrony Bank with QuickBooks: A Step-by-Step Integration Guide
You may want to see also
Frequently asked questions
Immunity acquired from a vaccine is the body's ability to resist or fight off a specific disease after being vaccinated. It occurs when the immune system recognizes and responds to a vaccine by producing antibodies and memory cells, preparing the body to combat the actual pathogen if exposed in the future.
A vaccine provides immunity by introducing a harmless form or part of a pathogen (such as a virus or bacterium) to the immune system. This triggers the production of antibodies and the development of memory cells, which allow the body to quickly recognize and neutralize the pathogen if it encounters it again.
Immunity from a vaccine is similar to natural immunity but is achieved without the risk of severe illness. Vaccines train the immune system to recognize and fight a pathogen, whereas natural immunity results from recovering from an actual infection, which can be dangerous or life-threatening.
The duration of immunity from a vaccine varies depending on the vaccine and the individual. Some vaccines provide lifelong immunity (e.g., measles), while others may require booster shots to maintain protection (e.g., tetanus). Factors like age, health, and the pathogen's characteristics also play a role.
Yes, immunity from a vaccine can wane over time, especially for vaccines that do not provide lifelong protection. This is why booster shots are sometimes necessary to reinforce the immune response and maintain adequate protection against the disease. Regular updates to vaccines may also be required for evolving pathogens.