Vaccines are essential tools in preventing infectious diseases, and they can be broadly categorized into two main types: live vaccines and killed vaccines. Live vaccines, also known as attenuated vaccines, contain a weakened form of the disease-causing pathogen, which is still capable of replicating but does not cause severe illness in healthy individuals. This type of vaccine mimics a natural infection, stimulating a strong and long-lasting immune response. Examples include the measles, mumps, and rubella (MMR) vaccine. On the other hand, killed vaccines, or inactivated vaccines, use pathogens that have been completely destroyed or rendered non-infectious through chemical or physical methods. These vaccines cannot replicate and often require adjuvants to enhance the immune response. Examples include the influenza and hepatitis A vaccines. Understanding the differences between live and killed vaccines is crucial for appreciating their unique mechanisms, efficacy, and appropriate use in public health strategies.
| Characteristics | Values |
|---|---|
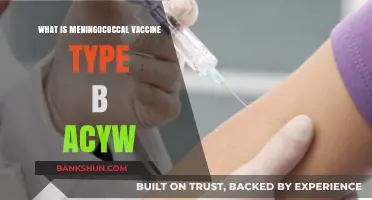
| Type | Live vaccines use weakened (attenuated) live pathogens, while killed (inactivated) vaccines use pathogens that have been destroyed or rendered non-infectious. |
| Immune Response | Live vaccines typically induce a stronger and more durable immune response, mimicking natural infection. Killed vaccines generally elicit a weaker response and may require adjuvants or booster doses. |
| Doses Required | Live vaccines often require fewer doses (e.g., 1-2 doses). Killed vaccines usually require multiple doses (e.g., 2-3 doses) and boosters. |
| Storage | Live vaccines often require refrigeration (2–8°C) and are more sensitive to heat and light. Killed vaccines are generally more stable and may not require strict refrigeration. |
| Safety | Live vaccines carry a small risk of causing disease in immunocompromised individuals. Killed vaccines are safer for immunocompromised individuals as they cannot cause the disease. |
| Examples | Live: Measles, Mumps, Rubella (MMR), Varicella (Chickenpox), Yellow Fever. Killed: Influenza (Flu), Polio (IPV), Hepatitis A, Rabies, COVID-19 (inactivated versions). |
| Cost | Live vaccines are often more expensive to produce due to the need for live pathogens. Killed vaccines are generally less expensive to manufacture. |
| Administration | Live vaccines are typically given via injection or orally. Killed vaccines are usually administered via injection. |
| Duration of Immunity | Live vaccines provide long-lasting immunity, often lifelong. Killed vaccines may require periodic boosters to maintain immunity. |
| Adjuvants | Killed vaccines often require adjuvants to enhance the immune response. Live vaccines do not typically need adjuvants. |
| Development Time | Live vaccines take longer to develop due to the need for attenuation. Killed vaccines can be developed more quickly as they involve inactivation of pathogens. |
Explore related products






What You'll Learn
- Live Vaccine Definition: Weakened pathogens, replicate in body, trigger strong immune response, provide long-lasting immunity
- Killed Vaccine Definition: Inactivated pathogens, cannot replicate, safer, often requires adjuvants or boosters
- Immune Response Comparison: Live vaccines induce robust immunity; killed vaccines rely on antibodies and memory cells
- Safety and Risks: Live vaccines may cause mild illness; killed vaccines are safer for immunocompromised individuals
- Examples: Live (MMR, varicella); Killed (influenza, hepatitis A, rabies)
![]()
Live Vaccine Definition: Weakened pathogens, replicate in body, trigger strong immune response, provide long-lasting immunity
Live vaccines are a cornerstone of modern immunology, leveraging the body's natural defense mechanisms to confer robust, long-lasting immunity. Unlike their inactivated counterparts, live vaccines contain weakened (attenuated) pathogens that retain the ability to replicate within the host. This replication mimics a natural infection, albeit at a reduced scale, triggering a vigorous immune response. For instance, the measles, mumps, and rubella (MMR) vaccine uses attenuated viruses to stimulate the production of antibodies and memory cells, offering protection that often lasts a lifetime. This approach is particularly effective because it engages both the innate and adaptive immune systems, creating a comprehensive defense against future encounters with the pathogen.
The process of attenuation is both precise and delicate. Scientists weaken pathogens through repeated culturing in non-human cells or by introducing specific genetic modifications. For example, the varicella-zoster virus in the chickenpox vaccine is attenuated by passing it through human and animal cell cultures, reducing its virulence while preserving its immunogenicity. This ensures the vaccine is safe for administration, typically in a single dose for children aged 12–15 months, with a booster at 4–6 years. However, because live vaccines contain active pathogens, they are contraindicated in immunocompromised individuals, pregnant women, and those with severe allergies to vaccine components. Careful screening and adherence to guidelines are essential to maximize safety and efficacy.
One of the most compelling advantages of live vaccines is their ability to provide long-term immunity with minimal doses. The oral polio vaccine (OPV), for instance, uses attenuated poliovirus strains to induce mucosal and systemic immunity after just two to three doses, administered starting at 6 weeks of age. This contrasts with killed vaccines, which often require multiple doses and adjuvants to achieve comparable protection. Live vaccines’ efficiency stems from their ability to replicate, amplifying the antigenic stimulus and closely mimicking natural infection. This makes them particularly effective for preventing highly contagious diseases like yellow fever, where a single dose of the live-attenuated vaccine provides lifelong immunity for most recipients.
Despite their strengths, live vaccines are not without limitations. Their requirement for refrigeration (the "cold chain") and potential for reversion to virulence, though rare, pose logistical and safety challenges. For example, the live-attenuated influenza vaccine (LAIV), administered intranasally, is less stable than its inactivated counterpart and must be stored between 2°C and 8°C. Additionally, live vaccines cannot be given simultaneously with immunoglobulins or blood products, as antibodies may neutralize the vaccine strains before they elicit an immune response. These considerations underscore the importance of proper handling, timing, and patient selection to ensure optimal outcomes.
In summary, live vaccines represent a powerful tool in preventive medicine, harnessing weakened pathogens to induce strong, durable immunity. Their ability to replicate within the body, coupled with their efficiency in dosing, makes them ideal for combating highly contagious diseases. However, their use requires careful consideration of contraindications and logistical constraints. By understanding their mechanisms and limitations, healthcare providers can maximize the benefits of live vaccines, contributing to global health and disease eradication efforts.
Mastering the Perris Banko Strap: A Step-by-Step Attachment Guide
You may want to see also
Explore related products






![]()
Killed Vaccine Definition: Inactivated pathogens, cannot replicate, safer, often requires adjuvants or boosters
Killed vaccines, also known as inactivated vaccines, are a cornerstone of modern immunization strategies, offering a safer alternative to live vaccines by using pathogens that have been rendered incapable of replication. This process involves treating viruses or bacteria with chemicals, heat, or radiation to destroy their ability to cause disease while preserving their antigenic properties. For instance, the inactivated polio vaccine (IPV) uses formaldehyde to inactivate the poliovirus, ensuring it cannot replicate in the body. This method significantly reduces the risk of adverse reactions, making killed vaccines particularly suitable for individuals with weakened immune systems, such as the elderly or those with chronic illnesses.
One of the key advantages of killed vaccines is their safety profile. Since the pathogens are dead, there is no risk of the vaccine causing the disease it aims to prevent, even in immunocompromised individuals. However, this safety comes with a trade-off: killed vaccines often elicit a weaker immune response compared to live vaccines. To compensate, they frequently require the addition of adjuvants—substances like aluminum salts that enhance the body’s immune reaction to the vaccine. For example, the hepatitis B vaccine contains an aluminum adjuvant to improve its effectiveness. Additionally, multiple doses or booster shots are often necessary to achieve and maintain immunity, as seen with the tetanus vaccine, which requires periodic boosters every 10 years.
Administering killed vaccines involves specific considerations to ensure optimal efficacy. Dosage and timing are critical, particularly for vaccines requiring multiple doses. For instance, the inactivated influenza vaccine is typically administered annually due to the virus’s evolving strains, while the rabies vaccine is given in a series of shots over several weeks after potential exposure. Age-specific guidelines also play a role; infants and young children often receive killed vaccines as part of their routine immunization schedule, such as the IPV, which is administered at 2, 4, 6, and 15–18 months of age. Adhering to these schedules is essential to build and sustain immunity.
Despite their safety, killed vaccines are not without limitations. Their inability to replicate means they may not provide the same level of long-lasting immunity as live vaccines, which mimic natural infection more closely. This is why boosters are often required. Additionally, the manufacturing process for killed vaccines can be more complex and costly, as it involves inactivating pathogens while maintaining their immunogenicity. However, their suitability for vulnerable populations and proven track record in preventing diseases like rabies, hepatitis A, and influenza make them an indispensable tool in public health.
In practical terms, individuals receiving killed vaccines should be aware of potential side effects, which are generally mild and include soreness at the injection site, low-grade fever, or fatigue. These symptoms typically resolve within a few days and can be managed with over-the-counter pain relievers. It’s also important to follow healthcare provider instructions regarding booster doses and to keep immunization records up to date. By understanding the unique characteristics of killed vaccines, individuals can make informed decisions about their health and contribute to broader community immunity.
TIAA Bank vs. EverBank: Are They the Same Institution?
You may want to see also
Explore related products






![]()
Immune Response Comparison: Live vaccines induce robust immunity; killed vaccines rely on antibodies and memory cells
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened forms of the pathogen, triggering a robust immune response that closely mimics a natural infection. This similarity to actual disease exposure prompts the body to mount a vigorous defense, involving both cellular and humoral immunity. The result is the production of long-lasting memory cells, ensuring rapid recognition and neutralization of the pathogen upon future encounters. For instance, a single dose of the live yellow fever vaccine provides lifelong immunity in 95% of recipients, showcasing the potency of this approach. This method is particularly effective in healthy individuals, especially children, whose immune systems are primed to respond aggressively.
In contrast, killed vaccines, like the inactivated polio vaccine (IPV), rely on inactivated pathogens to stimulate immunity. Without the ability to replicate, these vaccines primarily activate the humoral immune response, leading to the production of antibodies. While this response is crucial for neutralizing toxins and preventing infection, it often requires multiple doses and adjuvants to enhance effectiveness. For example, the IPV is typically administered in a series of three to four doses, starting at two months of age, to ensure adequate antibody levels. Killed vaccines are safer for immunocompromised individuals, as there is no risk of the pathogen reverting to a virulent form.
The immune response to live vaccines is characterized by its breadth and durability. These vaccines not only generate antibodies but also activate cytotoxic T cells, which are essential for eliminating infected cells. This dual-pronged approach ensures a more comprehensive defense mechanism. For instance, the live varicella vaccine, given as two doses starting at 12 months, provides over 90% protection against chickenpox and significantly reduces the risk of complications. However, live vaccines are contraindicated in pregnant women and those with severe immunodeficiency due to the theoretical risk of the attenuated pathogen causing disease.
Killed vaccines, while less likely to induce cellular immunity, are invaluable in specific contexts. They are often used for pathogens that cannot be safely attenuated or in populations where even a minimal risk of vaccine-induced disease is unacceptable. For example, the killed influenza vaccine is annually administered to millions of individuals, including the elderly and those with chronic conditions, to reduce the burden of seasonal flu. Its reliance on antibodies necessitates frequent updates to match circulating strains, highlighting the trade-off between safety and adaptability.
In practice, the choice between live and killed vaccines depends on the pathogen, the target population, and the desired immune outcome. Live vaccines offer unparalleled protection but require careful consideration of contraindications. Killed vaccines provide a safer alternative, albeit with a more limited immune response. For optimal protection, healthcare providers must weigh these factors, ensuring that vaccination strategies align with individual needs and public health goals. For instance, travelers to endemic areas might prioritize live vaccines for diseases like yellow fever, while routine childhood immunizations often include a mix of both types to maximize coverage and safety.
Withdrawing 1 Crore: A Step-by-Step Bank Withdrawal Guide
You may want to see also
Explore related products






![]()
Safety and Risks: Live vaccines may cause mild illness; killed vaccines are safer for immunocompromised individuals
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened forms of the virus that trigger a robust immune response. While highly effective, they carry a small risk of causing mild illness resembling the disease they prevent. For instance, the MMR vaccine can occasionally lead to a low-grade fever or rash in recipients. This occurs because the attenuated virus replicates minimally in the body, stimulating immunity without causing severe disease. However, this very mechanism makes live vaccines less suitable for individuals with compromised immune systems, as their bodies may struggle to control even the weakened virus.
Killed (inactivated) vaccines, like the injectable flu shot or the hepatitis A vaccine, use viruses that have been destroyed and cannot replicate. This design eliminates the risk of the vaccine causing the disease, making them safer for immunocompromised individuals, pregnant people, and those with specific medical conditions. For example, the inactivated polio vaccine (IPV) is recommended over the live oral polio vaccine (OPV) for individuals with HIV or cancer, as it poses no risk of viral replication. However, killed vaccines often require multiple doses and adjuvants to achieve comparable immunity, as they typically elicit a weaker initial response.
For immunocompromised patients, the choice between live and killed vaccines is critical. Live vaccines, such as the varicella (chickenpox) vaccine, are generally contraindicated in this population due to the risk of severe complications. Instead, healthcare providers opt for killed alternatives, like the pneumococcal polysaccharide vaccine (PPSV23), which protects against pneumonia without the risk of viral replication. Practical tips include ensuring patients are up to date on all killed vaccines before starting immunosuppressive therapies and consulting an immunologist for personalized recommendations.
A comparative analysis reveals that while live vaccines offer durable immunity with fewer doses, their safety profile limits their use in vulnerable populations. Killed vaccines, though requiring boosters, provide a safer option for those at risk. For instance, the live shingles vaccine (Zostavax) is not recommended for individuals over 60 with weakened immunity, whereas the newer recombinant shingles vaccine (Shingrix), though not strictly "killed," avoids live virus and is safer for this group. This highlights the importance of tailoring vaccine selection to individual health status.
In conclusion, understanding the safety and risks of live versus killed vaccines is essential for informed decision-making. While live vaccines may cause mild illness in healthy individuals, their potential complications in immunocompromised patients necessitate the use of killed alternatives. Healthcare providers must weigh efficacy, safety, and patient-specific factors to optimize vaccination strategies. Practical steps include reviewing medical histories, staying informed about contraindications, and prioritizing killed vaccines for at-risk groups to ensure both protection and safety.
Is a Bank Job Haram in Islam? Exploring Islamic Financial Ethics
You may want to see also
Explore related products






![]()
Examples: Live (MMR, varicella); Killed (influenza, hepatitis A, rabies)
Live vaccines, such as the MMR (measles, mumps, rubella) and varicella (chickenpox) vaccines, contain weakened forms of the virus that trigger a robust immune response without causing the disease. For instance, the MMR vaccine is typically administered in two doses: the first at 12–15 months and the second at 4–6 years. This schedule ensures long-term immunity, with studies showing over 95% effectiveness after the second dose. Similarly, the varicella vaccine is given in two doses, starting at 12–15 months, and provides approximately 90% protection against severe disease. These live vaccines mimic natural infection, often conferring lifelong immunity with minimal side effects, such as mild fever or rash.
In contrast, killed vaccines, like those for influenza, hepatitis A, and rabies, use inactivated viruses or their components to stimulate immunity. The influenza vaccine, for example, is updated annually to match circulating strains and is recommended for everyone aged 6 months and older. It is particularly crucial for high-risk groups, such as the elderly and immunocompromised individuals. The hepatitis A vaccine, administered in two doses 6–12 months apart, offers nearly 100% protection and is advised for travelers to endemic regions and those with chronic liver disease. The rabies vaccine, while rarely needed, is a lifesaver for those exposed to the virus, requiring a series of shots over 14 days to prevent the invariably fatal disease.
Comparing these two categories, live vaccines generally provide stronger, longer-lasting immunity but are contraindicated in immunocompromised individuals due to the risk of the virus reactivating. Killed vaccines, while safer for vulnerable populations, often require booster doses to maintain protection. For example, the influenza vaccine must be repeated yearly due to viral mutation, whereas the MMR vaccine typically confers lifelong immunity after two doses. This distinction highlights the importance of tailoring vaccine choice to the recipient’s health status and risk factors.
Practical considerations also differ between live and killed vaccines. Live vaccines, like varicella, should be spaced at least 4 weeks apart if not administered simultaneously, as concurrent administration can interfere with their effectiveness. Killed vaccines, such as hepatitis A and rabies, can be given concurrently with other vaccines without issue. Additionally, killed vaccines are often preferred in outbreak settings because they pose no risk of viral shedding, making them safer for community-wide use. Understanding these nuances helps healthcare providers optimize vaccination strategies for individual and public health.
Ultimately, the choice between live and killed vaccines depends on the specific disease, the recipient’s immune status, and the desired duration of protection. Live vaccines, exemplified by MMR and varicella, excel in providing durable immunity with minimal doses but require careful consideration of contraindications. Killed vaccines, such as influenza and hepatitis A, offer versatility and safety, particularly for at-risk populations, though they may demand more frequent administration. By leveraging the strengths of each type, healthcare systems can effectively prevent a wide range of diseases, from childhood infections to global health threats like rabies.
Does the Fed Interfere with Daily Bank Operations? A Deep Dive
You may want to see also
Frequently asked questions
A live vaccine contains a weakened (attenuated) form of the virus or bacteria that causes a disease. It stimulates a strong immune response, often providing long-lasting immunity with just one or two doses.
A killed vaccine contains inactivated (dead) forms of the virus or bacteria. It is safer for individuals with weakened immune systems but may require multiple doses or booster shots to maintain immunity.
Live vaccines mimic a natural infection, triggering a robust immune response involving both antibodies and T-cells. Killed vaccines primarily stimulate antibody production and may not activate T-cells as effectively.
Killed vaccines are generally safer because they cannot cause the disease they protect against. Live vaccines, while highly effective, carry a small risk of causing mild or severe disease in immunocompromised individuals.