The rollout of COVID-19 vaccines has been a critical step in combating the pandemic, with priority initially given to high-risk groups such as the elderly, healthcare workers, and those with underlying health conditions. As vaccination rates increase and supply becomes more stable, attention is now turning to the next age group eligible for immunization. This decision is guided by public health strategies aimed at maximizing protection and minimizing transmission, often focusing on younger populations who remain unvaccinated. Determining the next age group involves careful consideration of factors like disease prevalence, societal impact, and vaccine safety and efficacy in different demographics. Announcements regarding eligibility expansions are typically made by health authorities based on the latest data and recommendations from medical experts.
Explore related products






What You'll Learn
![]()
Eligibility criteria for next age group
As countries progress through their vaccination rollouts, the question of which age group will be prioritized next becomes increasingly pertinent. The eligibility criteria for the next age group are typically determined by a combination of factors, including the availability of vaccine doses, the vulnerability of the population, and the potential impact on public health. For instance, in many countries, the initial focus was on healthcare workers and the elderly, followed by individuals with underlying health conditions. The next logical step often involves expanding eligibility to younger age groups, but this decision is not arbitrary.
From an analytical perspective, the eligibility criteria for the next age group must consider the balance between risk and benefit. Younger individuals generally face lower risks from COVID-19 compared to older adults, but they can still contribute significantly to community transmission. For example, the 12-15 age group is often prioritized after the elderly and high-risk populations because they are more socially active and likely to spread the virus in school settings. Vaccinating this group can help reduce outbreaks and maintain educational continuity. Dosage adjustments are also crucial; for Pfizer-BioNTech, the same dosage as adults (30 µg) is administered to those aged 12 and above, while Moderna’s vaccine is typically given at a lower dose for younger age groups in some countries.
Instructively, when determining eligibility for the next age group, health authorities often follow a step-by-step approach. First, they assess the vaccination coverage in higher-risk groups to ensure sufficient protection. Second, they evaluate the epidemiological data to identify age groups contributing most to transmission. Third, they consider logistical factors, such as vaccine supply and distribution capabilities. For parents and guardians, practical tips include staying informed about local health department announcements, pre-registering for vaccination appointments if possible, and preparing children for the process by explaining what to expect. It’s also essential to follow post-vaccination guidelines, such as monitoring for side effects and scheduling the second dose if applicable.
Persuasively, expanding eligibility to the next age group is not just a public health decision but a societal one. Vaccinating younger populations accelerates the path to herd immunity, reducing the virus’s ability to circulate and mutate. For instance, the 16-24 age group, often overlooked due to lower hospitalization rates, plays a critical role in community spread, particularly in social and workplace settings. By prioritizing this group, countries can mitigate outbreaks in densely populated areas and protect vulnerable individuals who may not mount a full immune response to the vaccine. This approach aligns with the principle of collective responsibility, where individual actions contribute to broader societal well-being.
Comparatively, different countries adopt varying strategies for determining the next eligible age group. Some, like the United States and Canada, follow a linear progression, starting with older adults and gradually lowering the age threshold. Others, such as Israel and the UK, prioritize based on real-time data, adjusting eligibility criteria in response to emerging variants or localized outbreaks. For example, Israel initially focused on the 60+ age group but quickly expanded to younger populations once sufficient coverage was achieved in high-risk groups. This adaptive approach highlights the importance of flexibility in vaccination strategies, ensuring that resources are allocated where they are most needed.
In conclusion, the eligibility criteria for the next age group are shaped by a complex interplay of health risks, transmission dynamics, and logistical considerations. By understanding these factors and staying informed, individuals can better navigate the vaccination process and contribute to the global effort to control the pandemic. Whether through analytical assessments, instructive guidelines, persuasive arguments, or comparative insights, the goal remains clear: to protect as many people as possible and restore a sense of normalcy to communities worldwide.
Key Bank Discount Brokerage Services: What You Need to Know
You may want to see also
Explore related products






![]()
Vaccine types approved for younger populations
As global vaccination efforts expand, the focus has shifted to younger age groups, with regulatory bodies approving specific vaccine types for children and adolescents. The Pfizer-BioNTech COVID-19 vaccine, for instance, is authorized for individuals aged 5 and older, with a lower dosage (10 micrograms) administered to children aged 5-11, compared to the 30-microgram dose for those 12 and above. This tailored approach ensures safety and efficacy across different age categories.
Consider the Moderna COVID-19 vaccine, which has been approved for adolescents aged 12-17 in some countries, with ongoing trials for younger children. The dosage remains consistent at 50 micrograms for this age group, but the interval between doses may be extended to optimize immune response. Parents should consult healthcare providers to understand the specific recommendations for their child’s age and health status. This individualized guidance is crucial for maximizing protection while minimizing potential side effects.
A comparative analysis reveals that mRNA vaccines, such as Pfizer-BioNTech and Moderna, are currently leading in approvals for younger populations due to their high efficacy and favorable safety profiles. In contrast, viral vector vaccines like AstraZeneca and Johnson & Johnson have been less frequently approved for children and adolescents, often due to rare but serious side effects in younger individuals. This highlights the importance of selecting vaccine types based on age-specific risk-benefit assessments.
For practical implementation, caregivers should follow these steps: schedule vaccinations during periods when children are less likely to experience stress or disruptions, ensure hydration before and after the appointment, and monitor for common side effects like fever or soreness. Keep a record of vaccination dates and dosages, as some vaccines may require boosters or additional doses. By staying informed and prepared, parents can contribute to a smoother vaccination experience for their children.
In conclusion, the approval of vaccines for younger populations is a critical step in achieving broader immunity, but it requires careful consideration of vaccine types, dosages, and age-specific guidelines. As more data becomes available, these recommendations may evolve, emphasizing the need for ongoing communication between healthcare providers and families. This proactive approach ensures that the next age group for vaccination receives the safest and most effective protection available.
Understanding CCD in Banking: Meaning, Function, and Importance Explained
You may want to see also
Explore related products



$18.59 $19.95



![]()
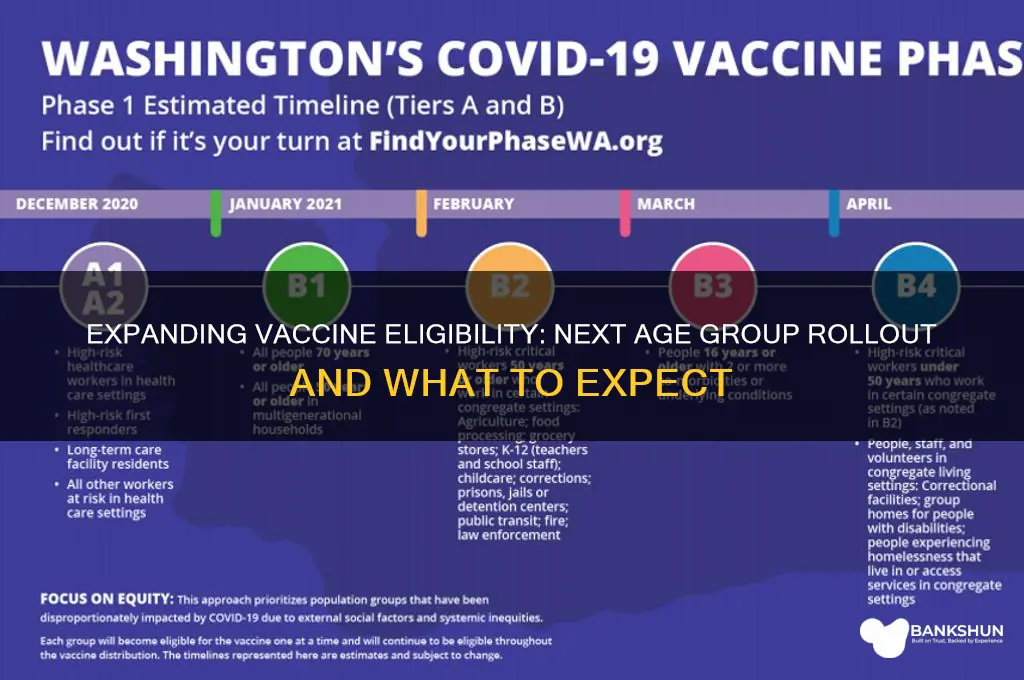
Rollout timeline and distribution plans
The next age group for vaccine rollout is a critical decision, often based on risk assessment, vaccine supply, and logistical feasibility. Typically, after prioritizing elderly populations and frontline workers, the focus shifts to younger demographics, such as adolescents and children. For instance, the Pfizer-BioNTech vaccine received emergency use authorization for individuals aged 12–15 in many countries, following successful clinical trials demonstrating safety and efficacy. This shift underscores the importance of a phased approach, balancing protection for vulnerable groups with broader community immunity.
A well-structured rollout timeline begins with identifying priority subgroups within the next age bracket. For example, adolescents with underlying health conditions might be vaccinated before their healthier peers. Distribution plans must account for school-based vaccination drives, leveraging existing health infrastructure to reach large numbers efficiently. In the U.S., the Centers for Disease Control and Prevention (CDC) recommended a two-dose regimen of 30 micrograms per dose for this age group, mirroring adult dosages but with careful monitoring for side effects. Such specificity ensures both safety and effectiveness in younger populations.
Logistics play a pivotal role in successful distribution. Unlike adult vaccinations, which often occur in hospitals or pharmacies, adolescent vaccines may be administered in schools or community centers. This requires coordination between health departments, educational institutions, and parents. For instance, Canada’s rollout included weekend clinics in schools, while some European countries integrated vaccination into routine health check-ups. Clear communication—such as informing parents about potential side effects like fatigue or fever—builds trust and encourages participation.
Comparatively, countries with higher vaccine hesitancy face unique challenges. In such cases, distribution plans must incorporate educational campaigns targeting parents and caregivers. For example, France paired its adolescent rollout with town hall meetings and social media campaigns featuring pediatricians. Meanwhile, nations with limited storage capabilities, such as those in warmer climates, prioritize vaccines like Pfizer’s, which requires ultra-cold storage, for urban areas while opting for more stable options like Moderna for rural regions.
Ultimately, the success of rollout timelines and distribution plans hinges on adaptability. Unforeseen factors—such as supply chain disruptions or new variants—may necessitate mid-course corrections. For instance, when India expanded its vaccination drive to include 15–18-year-olds, it initially faced shortages, prompting a shift to a staggered rollout by region. By learning from such examples, policymakers can design resilient strategies that ensure equitable access and maximize public health impact.
Vaccine Impact: Does Immunization Worsen Viral Outcomes?
You may want to see also
Explore related products






![]()
Safety and efficacy data for age group
As vaccine rollouts progress, the next age group to receive authorization often hinges on robust safety and efficacy data from clinical trials. For instance, the Pfizer-BioNTech COVID-19 vaccine was initially approved for individuals aged 16 and older, but subsequent trials involving 2,260 adolescents aged 12 to 15 demonstrated 100% efficacy in preventing symptomatic COVID-19. This data, including safety profiles showing mild to moderate side effects similar to those in older teens and adults, led to its emergency use authorization for this younger age group. Such trials are critical to ensuring vaccines are both safe and effective before expanding eligibility.
When evaluating safety data for a new age group, researchers scrutinize adverse events, immune responses, and dosage appropriateness. For example, Moderna’s COVID-19 vaccine trials for children aged 6 to 11 used a lower dose (50 micrograms, compared to 100 micrograms for adults) to minimize side effects while maintaining efficacy. This approach balances protection with tolerability, ensuring younger recipients experience fewer systemic reactions like fever or fatigue. Parents and caregivers should note that such adjustments are standard practice, reflecting the unique physiological needs of different age groups.
Efficacy data must also account for age-specific immune responses. Children and adolescents often mount stronger immune reactions to vaccines than adults, which can influence both dosing and expected outcomes. For instance, the Novavax COVID-19 vaccine trial in adolescents aged 12 to 17 showed robust antibody responses comparable to those in young adults, despite using the same dosage. This highlights the importance of age-stratified trials to confirm that immune responses align with protection levels observed in older populations.
Practical considerations for parents and healthcare providers include monitoring post-vaccination symptoms and adhering to recommended schedules. For vaccines requiring multiple doses, maintaining the prescribed interval (e.g., 3 to 4 weeks for Pfizer in adolescents) is crucial for optimal immunity. Additionally, transparency in communicating trial results builds trust, as seen in the detailed reporting of rare side effects like myocarditisisis myocardtexttextbitisises text text text content text text text text text text text text por public public.* safety text by practical
Returning to Christopher & Banks: A Step-by-Step Guide for Customers
You may want to see also
Explore related products






![]()
Parental consent requirements and guidelines
As countries expand vaccine eligibility to younger age groups, parental consent emerges as a critical yet complex requirement. For instance, the CDC's recent approval of the Pfizer-BioNTech vaccine for children aged 5-11 in the U.S. mandates written consent from a parent or guardian, a standard echoed in the UK's NHS guidelines for 12-15-year-olds. This raises questions about consent forms, legal guardianship, and the nuances of assent from minors themselves.
Consider the practicalities: consent forms often require detailed information, including the child’s full name, date of birth, and parent/guardian contact details. Some jurisdictions, like Canada, allow consent via digital platforms, while others insist on physical signatures. For divorced or separated parents, joint custody agreements may dictate who can provide consent, adding a layer of complexity. A key takeaway? Verify local regulations and prepare documentation in advance to avoid delays.
From an ethical standpoint, the concept of "assent" complements parental consent, particularly for adolescents. The American Academy of Pediatrics emphasizes that children aged 12 and older should be involved in the decision-making process, even if final approval rests with parents. This dual approach respects the child’s emerging autonomy while ensuring parental oversight. For example, a 14-year-old might express concerns about side effects, prompting a nurse to provide age-appropriate explanations before proceeding.
Comparatively, countries like Germany and France adopt a more flexible stance, allowing minors aged 16 and above to consent independently for medical procedures, including vaccination. This contrasts sharply with states like Texas, where parental consent is non-negotiable regardless of age. Such disparities highlight the need for global standardization, especially in cross-border scenarios. For parents traveling with children, carrying notarized consent letters could prove invaluable.
Finally, a persuasive argument for streamlining consent processes: simplifying requirements could boost vaccination rates among younger age groups. For instance, Spain’s use of SMS-based consent for 12-17-year-olds during its rollout exemplifies innovation. By reducing bureaucratic hurdles, health systems can focus on education and accessibility, ensuring that consent becomes a gateway, not a barrier, to protection.
Zelle Fee Charges: What PNC Bank Customers Need to Know
You may want to see also
Frequently asked questions
The next age group eligible for the COVID-19 vaccine depends on local health authority guidelines, but typically, after prioritizing elderly and high-risk populations, eligibility expands to younger adults and adolescents.
Eligibility for children under 12 depends on regulatory approval of vaccines for this age group, which varies by country and vaccine manufacturer.
The next age group for booster shots is usually determined after prioritizing older adults and immunocompromised individuals, with eligibility gradually expanding to younger age groups based on public health recommendations.
Updates on vaccine eligibility for the next age group are typically announced through official health department websites, local news, or direct communication from healthcare providers.