The various coronavirus vaccines developed to combat COVID-19 differ in their technology, efficacy, and administration. While mRNA vaccines like Pfizer-BioNTech and Moderna use genetic material to instruct cells to produce a harmless spike protein, viral vector vaccines such as AstraZeneca and Johnson & Johnson employ a modified virus to deliver genetic instructions. Additionally, inactivated vaccines like Sinovac and Sinopharm contain killed virus particles to trigger an immune response. These differences influence factors like storage requirements, dosing schedules, and potential side effects, making it essential to understand the unique characteristics of each vaccine to ensure informed decision-making and effective public health strategies.
| Characteristics | Values |
|---|---|
| Vaccine Type | mRNA (Pfizer-BioNTech, Moderna), Viral Vector (AstraZeneca, J&J), Protein Subunit (Novavax), Inactivated (Sinovac, Sinopharm) |
| Efficacy (Against Symptomatic Disease) | Pfizer: 95%, Moderna: 94.1%, AstraZeneca: 70-82%, J&J: 66-72%, Novavax: 90.4%, Sinovac: 51-83.5%, Sinopharm: 72-79% |
| Dose Regimen | Pfizer: 2 doses (21 days apart), Moderna: 2 doses (28 days apart), AstraZeneca: 2 doses (4-12 weeks apart), J&J: Single dose, Novavax: 2 doses (3-8 weeks apart), Sinovac: 2 doses (2-4 weeks apart), Sinopharm: 2 doses (3-4 weeks apart) |
| Storage Temperature | Pfizer: -90°C to -60°C, Moderna: -25°C to -15°C, AstraZeneca: 2°C to 8°C, J&J: 2°C to 8°C, Novavax: 2°C to 8°C, Sinovac: 2°C to 8°C, Sinopharm: 2°C to 8°C |
| Technology | Pfizer & Moderna: mRNA, AstraZeneca & J&J: Adenovirus vector, Novavax: Recombinant protein, Sinovac & Sinopharm: Inactivated virus |
| Approval Status (as of Oct 2023) | All approved by WHO for emergency use; Pfizer, Moderna, AstraZeneca, and J&J widely approved in multiple countries |
| Side Effects | Common: Pain at injection site, fatigue, headache, muscle pain, fever; Rare: Myocarditis (mRNA vaccines), Thrombosis with thrombocytopenia (AstraZeneca, J&J) |
| Booster Recommendations | mRNA boosters recommended after 6 months; AstraZeneca and J&J may require mRNA booster for enhanced immunity |
| Effectiveness Against Variants | Reduced efficacy against Omicron and Delta variants; boosters improve protection |
| Cost (Approximate) | Pfizer: $19.50/dose, Moderna: $32/dose, AstraZeneca: $2.50-$8.50/dose, J&J: $10/dose, Novavax: $16/dose, Sinovac: $10/dose, Sinopharm: $15/dose |
| Global Distribution | Pfizer and Moderna dominant in high-income countries; AstraZeneca, Sinovac, and Sinopharm widely used in low- and middle-income countries |
Explore related products






What You'll Learn
- Vaccine Types: mRNA, viral vector, protein subunit, and whole virus vaccines explained briefly
- Efficacy Rates: Comparison of effectiveness against infection, severe illness, and hospitalization
- Side Effects: Common reactions, severity, and differences across vaccine brands
- Dosage Schedules: Number of doses, intervals, and booster requirements for each vaccine
- Storage Needs: Temperature and handling differences impacting distribution and accessibility
![]()
Vaccine Types: mRNA, viral vector, protein subunit, and whole virus vaccines explained briefly
The COVID-19 pandemic spurred the development of multiple vaccine technologies, each with distinct mechanisms to trigger immunity. Understanding these differences empowers informed decisions about vaccination. Here's a breakdown of four key types:
MRNA vaccines, like Pfizer-BioNTech and Moderna, deliver genetic instructions for our cells to temporarily produce a harmless piece of the virus's spike protein. This protein triggers an immune response, preparing the body to fight the real virus. These vaccines boast high efficacy (around 95% after two doses) and require ultra-cold storage due to mRNA's fragility. Two doses, typically 3-4 weeks apart, are standard, with boosters recommended for sustained protection.
Viral vector vaccines, such as AstraZeneca and Johnson & Johnson, use a modified, harmless virus (the vector) to deliver genetic material coding for the spike protein. This material is then used by our cells to produce the protein, prompting an immune response. These vaccines are easier to store than mRNA types but have slightly lower efficacy (around 67-90%, depending on the vaccine and dosing regimen). A single dose is often sufficient for Johnson & Johnson, while AstraZeneca typically requires two doses, 4-12 weeks apart.
Protein subunit vaccines, exemplified by Novavax, directly inject a purified piece of the virus's spike protein, often combined with an adjuvant to enhance the immune response. This approach mimics natural infection without introducing any viral genetic material. Novavax demonstrates efficacy comparable to mRNA vaccines (around 90%) and can be stored in standard refrigerators, making it logistically advantageous. Two doses, 3-4 weeks apart, are typically administered.
Whole virus vaccines, like Sinopharm and Sinovac, use inactivated or weakened versions of the entire SARS-CoV-2 virus. This traditional approach exposes the immune system to the complete viral structure, triggering a broad immune response. Efficacy varies widely (50-90%, depending on the vaccine and study), and multiple doses (often three) are usually required for optimal protection.
Choosing the right vaccine depends on individual factors like age, health status, and availability. Consult healthcare professionals for personalized advice. Remember, all authorized COVID-19 vaccines significantly reduce the risk of severe illness, hospitalization, and death. Getting vaccinated, regardless of the type, is crucial for protecting yourself and your community.
Strategies to Streamline Bank Operations and Cut Costs Effectively
You may want to see also
Explore related products






![]()
Efficacy Rates: Comparison of effectiveness against infection, severe illness, and hospitalization
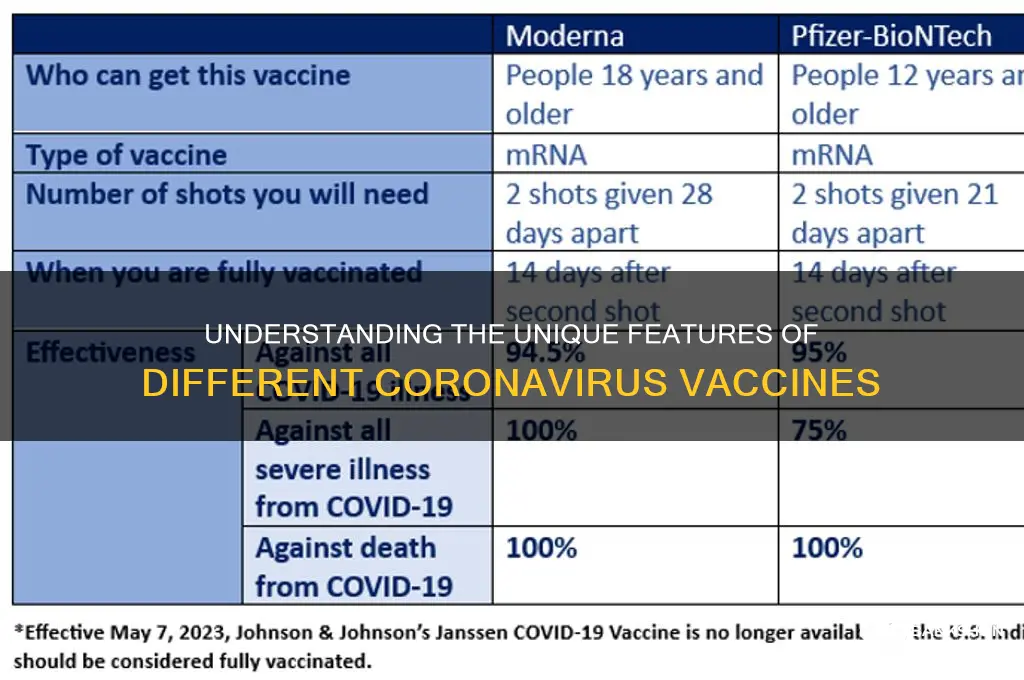
The efficacy of coronavirus vaccines varies significantly across different metrics: preventing infection, severe illness, and hospitalization. Clinical trials and real-world data reveal that no single vaccine dominates all three categories, making the choice of vaccine dependent on individual health needs and community transmission rates. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna initially demonstrated 95% efficacy against symptomatic infection in trials, but this figure dropped to around 60-70% against the Delta variant and even lower against Omicron, highlighting the impact of viral evolution on vaccine performance.
Consider the practical implications of these efficacy rates. A vaccine with high efficacy against infection, such as Pfizer’s 95% in trials, reduces the likelihood of transmitting the virus to others, making it a strong choice for individuals in high-contact professions or communities with low vaccination rates. However, all approved vaccines maintain robust protection against severe illness and hospitalization, typically above 90%, even against variants like Omicron. For example, a study in *The Lancet* found that two doses of AstraZeneca provided 92% protection against hospitalization from the Alpha variant, while Moderna’s booster restored efficacy against severe Omicron cases to over 90%.
When comparing vaccines, it’s crucial to factor in dosage and age-specific responses. Pfizer’s three-dose regimen for individuals over 12 years old enhances protection against infection and severe outcomes, particularly in older adults whose immune responses may wane faster. In contrast, Johnson & Johnson’s single-dose vaccine offers lower initial efficacy against infection (around 66%) but still provides strong protection against hospitalization (85% in trials). For immunocompromised individuals, a third dose of mRNA vaccines is recommended to achieve comparable protection levels, as their initial two-dose response may be suboptimal.
A persuasive argument for vaccination lies in the collective impact of efficacy rates. While no vaccine prevents infection entirely, especially with variants like Omicron, their ability to drastically reduce severe outcomes and hospitalizations alleviates strain on healthcare systems. For instance, countries with high vaccination rates, such as Israel, saw a 90% reduction in COVID-19 deaths during Omicron waves compared to unvaccinated populations. This underscores the importance of choosing a vaccine based on availability and personal risk factors rather than waiting for a “perfect” option.
In conclusion, understanding efficacy rates requires a nuanced approach. Vaccines differ in their ability to prevent infection versus severe illness, but all significantly reduce hospitalization risk. Practical considerations, such as dosing schedules and age-specific responses, further influence vaccine choice. By focusing on real-world data and individual needs, individuals can make informed decisions that maximize protection for themselves and their communities.
Is Your Bank ATM Chip-Enabled? What You Need to Know
You may want to see also
Explore related products






![]()
Side Effects: Common reactions, severity, and differences across vaccine brands
Side effects are the body's natural response to vaccination, signaling the immune system's activation. Across COVID-19 vaccine brands—Pfizer-BioNTech, Moderna, Johnson & Johnson (J&J), and others—common reactions include pain at the injection site, fatigue, headache, muscle pain, chills, fever, and nausea. These symptoms typically appear within 24–48 hours post-vaccination and resolve within a few days. For instance, both Pfizer and Moderna (mRNA vaccines) frequently cause arm soreness, while J&J’s viral vector vaccine often leads to more systemic effects like fever and body aches.
Severity varies by vaccine type and individual factors. mRNA vaccines (Pfizer and Moderna) tend to produce more intense side effects, particularly after the second dose, due to a robust immune response. For example, fever occurs in about 16% of Pfizer recipients after dose two, compared to 6% after dose one. Moderna’s higher dosage (100 µg vs. Pfizer’s 30 µg) correlates with slightly stronger reactions. J&J’s single-dose vaccine causes milder side effects overall but has a rare risk of blood clots with low platelets, primarily in women under 50. Novavax, a protein subunit vaccine, reports milder reactions, with fatigue and headache being the most common.
Age and health status influence side effect profiles. Younger individuals (18–55) generally experience more pronounced reactions than older adults (65+), likely due to a more active immune system. Pregnant individuals and those with compromised immunity may have milder responses but should consult healthcare providers for personalized advice. For children (5–11), Pfizer’s lower dose (10 µg) reduces side effects, with fever occurring in less than 1% of recipients.
Practical tips can mitigate discomfort. Over-the-counter pain relievers like acetaminophen or ibuprofen can ease pain and fever, but avoid taking them preemptively, as they may dampen immune response. Applying a cool, wet washcloth to the injection site and staying hydrated can help manage symptoms. Rest is crucial, especially if fatigue or fever occurs. Monitor for severe or persistent symptoms, such as difficulty breathing or chest pain, and seek medical attention immediately if they arise.
Understanding these differences empowers individuals to choose a vaccine aligned with their health needs and preferences. While side effects can be unpleasant, they are temporary and far outweighed by the protection against severe COVID-19. Each vaccine brand offers unique advantages, and the best choice is the one available and suitable for the individual. Always consult a healthcare provider for tailored advice, especially for specific medical conditions or concerns.
Is Jos. A. Bank a Good Suit Choice? A Comprehensive Review
You may want to see also
Explore related products






![]()
Dosage Schedules: Number of doses, intervals, and booster requirements for each vaccine
The Pfizer-BioNTech and Moderna mRNA vaccines both require two initial doses, but the interval between them differs: 21 days for Pfizer and 28 days for Moderna. This slight difference reflects the vaccines’ unique formulations and clinical trial designs. Both vaccines have demonstrated high efficacy after the second dose, but the optimal timing is crucial for maximizing immune response. For instance, delaying the second dose beyond the recommended interval may reduce the vaccine’s effectiveness, so adherence to the schedule is essential.
Booster requirements for these mRNA vaccines have evolved with emerging variants and waning immunity. Initially, boosters were recommended 6 months after the second dose for individuals aged 12 and older. However, in response to Omicron and its subvariants, the interval was shortened to 5 months for Pfizer and 6 months for Moderna. Additionally, a second booster (fourth dose) is now advised for individuals aged 50 and older or those with immunocompromised conditions, further emphasizing the dynamic nature of dosage schedules.
The Johnson & Johnson (J&J) vaccine stands out as a single-dose regimen, offering convenience for those hesitant about multiple shots. However, data on waning immunity led health authorities to recommend a booster dose at least 2 months after the initial shot. This adjustment highlights the vaccine’s unique position—while one dose provides initial protection, a booster significantly enhances immunity, particularly against severe disease and hospitalization.
AstraZeneca’s viral vector vaccine, widely used outside the U.S., typically requires two doses with an interval of 8 to 12 weeks. This extended gap was found to improve efficacy compared to shorter intervals. Booster recommendations vary by country, with some advising an mRNA vaccine as the third dose for broader immune stimulation. This hybrid approach underscores the flexibility and adaptability of vaccination strategies.
Practical tips for navigating dosage schedules include setting reminders for follow-up doses, ensuring access to vaccination sites, and staying informed about updated guidelines. For parents, noting that Pfizer is the only vaccine approved for children as young as 6 months (with a three-dose series for ages 6 months to 4 years) is critical. Always consult healthcare providers for personalized advice, especially for immunocompromised individuals or those with specific health conditions. Understanding these schedules empowers individuals to make informed decisions and contribute to collective immunity.
Contact Fifth Third Bank: Easy Ways to Reach Customer Service
You may want to see also
Explore related products






![]()
Storage Needs: Temperature and handling differences impacting distribution and accessibility
One of the most critical yet often overlooked aspects of coronavirus vaccines is their storage requirements, which vary dramatically across types. For instance, the Pfizer-BioNTech mRNA vaccine demands ultra-cold storage at -70°C (-94°F), a logistical nightmare for many regions lacking specialized freezers. In contrast, the Moderna mRNA vaccine is more forgiving, stable at -20°C (-4°F) for up to six months, and can even be refrigerated at 2°C to 8°C (36°F to 46°F) for 30 days. These differences aren’t trivial—they dictate where and how quickly vaccines can be distributed, particularly in low-resource settings or remote areas.
Consider the adenovirus-based vaccines, such as Oxford-AstraZeneca and Johnson & Johnson, which offer a stark contrast in storage needs. Both can be kept in standard refrigerators at 2°C to 8°C, making them far more accessible for global distribution. This simplicity has been a game-changer for countries with limited infrastructure, enabling broader vaccination campaigns. However, even these vaccines have nuances: Johnson & Johnson’s single-dose regimen reduces handling complexity compared to AstraZeneca’s two-dose schedule, which requires careful tracking and storage over time.
The implications of these storage differences extend beyond logistics to equity. Ultra-cold chain requirements disproportionately disadvantage low- and middle-income countries, where such facilities are scarce. For example, Pfizer’s vaccine initially struggled to reach rural areas in Africa, while AstraZeneca’s was widely adopted due to its ease of storage. This disparity highlights how temperature and handling requirements can inadvertently create a two-tiered system of vaccine accessibility, exacerbating global health inequalities.
Practical tips for healthcare providers and distributors are essential. For mRNA vaccines, investing in portable ultra-cold freezers or dry ice solutions can mitigate storage challenges, though these come with added costs. For adenovirus vaccines, ensuring consistent refrigeration and minimizing temperature fluctuations is key. Additionally, training staff on proper handling—such as avoiding light exposure for some vials or maintaining precise temperature logs—can prevent wastage. These steps, though seemingly small, are critical to maximizing vaccine efficacy and reach.
Ultimately, the storage needs of coronavirus vaccines are not just technical details—they shape the entire landscape of global vaccination efforts. As new vaccines emerge, manufacturers must prioritize stability at higher temperatures to improve accessibility. Until then, understanding and adapting to these differences remains a cornerstone of successful distribution, ensuring that life-saving doses reach those who need them most, regardless of geography or infrastructure.
Kellogg's Bank Reconciliation Frequency: A Comprehensive Financial Overview
You may want to see also
Frequently asked questions
mRNA vaccines (like Pfizer-BioNTech and Moderna) use genetic material to instruct cells to produce a harmless piece of the virus’s spike protein, triggering an immune response. Viral vector vaccines (like Johnson & Johnson and AstraZeneca) use a modified, harmless virus to deliver genetic instructions to cells to produce the spike protein, prompting immunity.
Most coronavirus vaccines require two doses for full protection (e.g., Pfizer-BioNTech, Moderna, AstraZeneca). However, some, like the Johnson & Johnson vaccine, are designed as a single-dose regimen. Booster shots may also be recommended depending on the vaccine and evolving public health guidance.
Common side effects are similar across vaccines (e.g., pain at the injection site, fatigue, headache). However, mRNA vaccines (Pfizer-BioNTech, Moderna) are more likely to cause mild to moderate side effects after the second dose, while viral vector vaccines (Johnson & Johnson, AstraZeneca) have a rare risk of blood clots or other specific adverse events. Always consult healthcare providers for personalized advice.