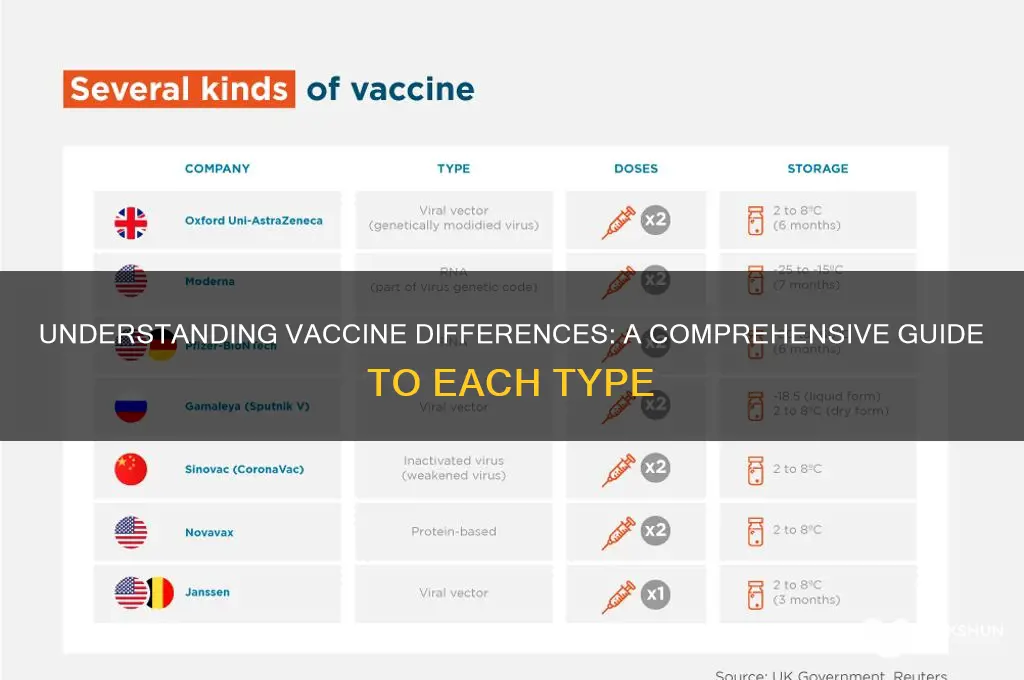
Vaccines are essential tools in preventing infectious diseases, but they differ significantly in their composition, mechanism of action, and target pathogens. Each vaccine is specifically designed to protect against a particular disease, such as influenza, measles, or COVID-19, by stimulating the immune system to recognize and combat the causative agent. The key differences lie in the type of vaccine technology used, which can include live-attenuated, inactivated, mRNA, viral vector, or protein subunit vaccines. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna deliver genetic instructions to cells to produce a harmless viral protein, triggering an immune response, while viral vector vaccines like AstraZeneca and Johnson & Johnson use a modified virus to transport genetic material into cells. Understanding these distinctions is crucial for informed decision-making and appreciating the tailored approach each vaccine takes to safeguard public health.
Explore related products




What You'll Learn
- Vaccine Types: Live-attenuated, inactivated, mRNA, viral vector, protein subunit, toxin, and conjugate vaccines
- Immune Response: Differences in how each vaccine triggers immunity in the body
- Efficacy Rates: Varying effectiveness against disease prevention and severity reduction
- Storage Needs: Unique temperature and handling requirements for each vaccine type
- Side Effects: Common and rare adverse reactions specific to different vaccines
![]()
Vaccine Types: Live-attenuated, inactivated, mRNA, viral vector, protein subunit, toxin, and conjugate vaccines
Vaccines are not one-size-fits-all; they are tailored to combat specific pathogens using distinct mechanisms. Live-attenuated vaccines, like the measles-mumps-rubella (MMR) shot, use weakened viruses to trigger a robust immune response. These vaccines mimic natural infection without causing disease, offering long-lasting immunity often after just one or two doses. However, they are contraindicated for immunocompromised individuals due to the risk of the virus reverting to its virulent form. For example, the MMR vaccine is administered at 12–15 months and 4–6 years, providing lifelong protection against three serious diseases.
In contrast, inactivated vaccines, such as the injectable polio vaccine (IPV), contain killed pathogens incapable of replicating. While safer for those with weakened immune systems, they typically require multiple doses and booster shots to maintain immunity. The IPV, for instance, is given in a series of four doses starting at 2 months of age, with a booster at 4–6 years. This type of vaccine is less likely to cause adverse reactions but may not elicit as strong an immune response as live-attenuated vaccines.
MRNA vaccines, like Pfizer-BioNTech and Moderna’s COVID-19 shots, represent a revolutionary approach. They deliver genetic instructions to cells, prompting them to produce a harmless viral protein that triggers an immune response. These vaccines are highly effective, with Pfizer’s requiring two doses 21 days apart for adults, while Moderna’s doses are spaced 28 days apart. Their rapid development and adaptability make them ideal for emerging pathogens, though they require ultra-cold storage, which can pose logistical challenges.
Viral vector vaccines, such as Johnson & Johnson’s COVID-19 vaccine, use a modified harmless virus to deliver genetic material into cells. This single-dose vaccine is particularly advantageous in hard-to-reach areas due to its stability at standard refrigeration temperatures. However, rare but serious side effects, like thrombosis with thrombocytopenia syndrome (TTS), have been reported, primarily in women under 50. This highlights the importance of weighing risks and benefits when choosing a vaccine.
Protein subunit vaccines, like Novavax’s COVID-19 vaccine, contain only specific pieces of a pathogen, such as its spike protein. These vaccines are highly targeted and safe, as they cannot cause infection. Novavax’s two-dose regimen, administered 21 days apart, is suitable for individuals hesitant about newer technologies like mRNA. Their stability at standard refrigeration temperatures also simplifies distribution.
Toxin and conjugate vaccines address bacterial infections by neutralizing harmful toxins or targeting bacterial coatings. For example, the DTaP vaccine protects against diphtheria, tetanus, and pertussis by including inactivated toxins (toxoids) and bacterial components. Conjugate vaccines, like the pneumococcal conjugate vaccine (PCV13), link a weak antigen to a strong one, enhancing the immune response in infants and young children. PCV13 is administered in a series of four doses starting at 2 months, safeguarding against 13 strains of pneumococcal bacteria.
Each vaccine type offers unique advantages and considerations, tailored to the pathogen and population it serves. Understanding these differences empowers individuals to make informed decisions about their health and protection.
Exploring the Largest Banks in the USA: A Comprehensive Overview
You may want to see also
Explore related products






![]()
Immune Response: Differences in how each vaccine triggers immunity in the body
Vaccines are not one-size-fits-all; they harness distinct mechanisms to prime the immune system against pathogens. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna introduce genetic material that instructs cells to produce a harmless spike protein, mimicking SARS-CoV-2. This triggers an adaptive immune response, with B cells producing antibodies and T cells preparing for future encounters. In contrast, viral vector vaccines such as Johnson & Johnson and AstraZeneca use a modified adenovirus to deliver genetic instructions, eliciting a similar but slightly different immune profile due to the vector’s role in antigen presentation. Understanding these differences is crucial for tailoring vaccination strategies to specific populations, such as immunocompromised individuals or older adults.
Consider the dosage and administration nuances that further differentiate immune responses. mRNA vaccines typically require two doses, spaced 3–4 weeks apart for Pfizer or 4–8 weeks for Moderna, to achieve optimal immunity. Viral vector vaccines often require a single dose, but a booster may be recommended for enhanced protection. Protein subunit vaccines, like Novavax, deliver stabilized spike proteins directly, paired with an adjuvant to amplify the immune response. This approach is particularly effective for those with mRNA vaccine hesitancy or contraindications, as it avoids genetic material altogether. Each vaccine’s dosing regimen and delivery method influence the timing and magnitude of the immune response, making them suitable for diverse age groups and health conditions.
A comparative analysis reveals how these vaccines engage innate and adaptive immunity differently. mRNA vaccines excel at rapidly inducing high levels of neutralizing antibodies, a key defense against viral entry. Viral vector vaccines, however, tend to stimulate a stronger T cell response, which is vital for clearing infected cells. Protein subunit vaccines strike a balance, offering robust antibody production with minimal risk of side effects, thanks to their non-replicating nature. For example, Novavax’s use of Matrix-M adjuvant enhances antigen uptake by immune cells, making it highly effective even at lower doses. These variations highlight the importance of vaccine choice based on individual immune status and disease prevalence.
Practical tips for maximizing immune response include adhering to recommended dosing intervals and considering booster shots, especially for mRNA and viral vector vaccines. For older adults or those with weakened immunity, protein subunit vaccines may be preferable due to their safety profile and adjuvant-enhanced efficacy. Additionally, staying hydrated and maintaining a balanced diet post-vaccination can support immune function. While all vaccines aim to prevent severe illness, their distinct mechanisms mean that side effects, such as fatigue or injection site pain, may vary. Recognizing these differences empowers individuals to make informed decisions and fosters trust in vaccination programs.
Ordering Simulated Blood Bank Bags: A Comprehensive Guide for Medical Training
You may want to see also
Explore related products





![]()
Efficacy Rates: Varying effectiveness against disease prevention and severity reduction
Vaccine efficacy rates are not one-size-fits-all. They vary widely depending on the disease, vaccine type, and population. For instance, the Pfizer-BioNTech COVID-19 vaccine demonstrated 95% efficacy in preventing symptomatic infection in clinical trials, while the Johnson & Johnson vaccine showed 66% efficacy globally but 72% in the U.S. These numbers highlight a critical point: efficacy rates are context-specific, influenced by factors like circulating virus variants and regional healthcare infrastructure. Understanding these nuances is essential for informed decision-making, especially when comparing vaccines for the same disease.
Consider the influenza vaccine, which typically ranges from 40% to 60% efficacy annually. This variability stems from the need to predict dominant strains months in advance, a process that can miss the mark. For older adults, the CDC recommends higher-dose or adjuvanted flu vaccines, which have shown efficacy rates up to 24% higher than standard-dose vaccines in this age group. This example underscores the importance of tailoring vaccines to specific demographics and health needs, as efficacy rates can differ significantly across populations.
Efficacy rates also extend beyond disease prevention to severity reduction. The Moderna COVID-19 vaccine, for instance, demonstrated 93% efficacy in preventing symptomatic infection but was even more effective—over 98%—in preventing severe disease requiring hospitalization. Similarly, the HPV vaccine Gardasil 9 has shown nearly 100% efficacy in preventing cervical precancers caused by the nine HPV types it targets. These examples illustrate how vaccines can serve dual purposes: reducing the likelihood of infection and minimizing the severity of breakthrough cases.
Practical considerations further complicate the efficacy landscape. Booster doses, for example, can significantly enhance protection. A third dose of the Pfizer-BioNTech COVID-19 vaccine increased antibody levels 25-fold in individuals over 55, restoring efficacy against symptomatic infection to over 90%. Timing matters too: the shingles vaccine Shingrix requires two doses, administered 2 to 6 months apart, to achieve its 97% efficacy rate in adults over 50. Adhering to recommended schedules and dosages is crucial for maximizing vaccine effectiveness.
In conclusion, efficacy rates are a dynamic measure of vaccine performance, shaped by disease characteristics, vaccine design, and population factors. While high efficacy is ideal, even vaccines with moderate rates, like the 66% effective Johnson & Johnson COVID-19 vaccine, play a vital role in public health by reducing severe outcomes and hospitalizations. By understanding these variations, individuals and healthcare providers can make more informed choices, ensuring the best possible protection against preventable diseases.
Understanding the Role of a Bank Financial Analyst: Key Responsibilities and Skills
You may want to see also
Explore related products






![]()
Storage Needs: Unique temperature and handling requirements for each vaccine type
Vaccines are not one-size-fits-all, and neither are their storage needs. Each vaccine type demands specific temperature and handling conditions to maintain potency and safety. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna require ultra-cold storage, typically between -60°C and -80°C, due to their lipid nanoparticle components. This poses logistical challenges, especially in regions with limited infrastructure, necessitating specialized freezers and careful transportation protocols. In contrast, viral vector vaccines such as AstraZeneca and Johnson & Johnson are more stable, with storage temperatures ranging from 2°C to 8°C, similar to standard refrigerator conditions. This makes them more accessible for widespread distribution, particularly in low-resource settings.
The handling requirements extend beyond temperature. mRNA vaccines, once thawed, have a limited shelf life—Pfizer’s vaccine must be used within 5 days when stored at 2°C to 8°C, while Moderna’s can last up to 30 days under the same conditions. This demands precise inventory management to minimize waste. Inactivated vaccines, like Sinovac and Sinopharm, also require refrigeration but are generally more forgiving, with longer stability periods once opened. However, they must be protected from light and agitation, which can degrade their efficacy. Understanding these nuances is critical for healthcare providers to ensure vaccines remain viable from production to administration.
Consider the practical implications for vaccination campaigns. For a mobile clinic administering Pfizer’s vaccine, a portable ultra-low freezer and a backup power source are essential to prevent temperature excursions during transport. In contrast, a rural health center distributing AstraZeneca vaccines might rely on standard refrigeration units, reducing costs and complexity. Diluent requirements also vary—some vaccines, like Pfizer’s, need to be mixed with a specific diluent immediately before use, while others come pre-filled and ready to administer. These differences highlight the need for tailored training and resources for healthcare workers.
A comparative analysis reveals that storage needs directly impact vaccine accessibility and equity. Ultra-cold chain requirements limit the reach of mRNA vaccines, particularly in developing countries, whereas the stability of viral vector and inactivated vaccines makes them more suitable for global distribution. For example, the COVAX initiative prioritizes vaccines with less stringent storage needs to ensure equitable access. However, as technology advances, innovations like thermal-stable formulations could reduce these disparities. Until then, careful planning and resource allocation are crucial to meet the unique storage demands of each vaccine type.
In conclusion, the storage and handling requirements of vaccines are as diverse as the technologies behind them. From ultra-cold freezers to standard refrigerators, each vaccine type demands specific conditions to preserve its efficacy. Healthcare systems must adapt by investing in appropriate infrastructure, training staff, and optimizing supply chains. By addressing these challenges, we can ensure that vaccines reach those who need them most, regardless of their storage complexities. Practical tips, such as using digital temperature monitors and maintaining detailed inventory logs, can further enhance compliance and reduce waste. Ultimately, understanding and meeting these unique storage needs is a cornerstone of successful vaccination programs.
Is Synchrony Bank Affiliated with American Express? Unraveling the Connection
You may want to see also
Explore related products






![]()
Side Effects: Common and rare adverse reactions specific to different vaccines
Vaccines, while crucial for preventing diseases, come with distinct side effect profiles that vary by type. Understanding these differences is essential for informed decision-making and managing expectations. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna, which use genetic material to trigger an immune response, commonly cause mild to moderate reactions such as fatigue, headache, and muscle pain, particularly after the second dose. These symptoms typically resolve within a few days and are a sign of the immune system responding as intended. In contrast, viral vector vaccines like Johnson & Johnson and AstraZeneca, which use a modified virus to deliver genetic instructions, are more frequently associated with rare but serious side effects, such as thrombosis with thrombocytopenia syndrome (TTS), occurring in approximately 7 per 1 million vaccinated women aged 18–49.
Analyzing these side effects reveals patterns tied to vaccine mechanisms. For example, the high efficacy of mRNA vaccines (94–95% in trials) correlates with their higher likelihood of causing systemic reactions, as they provoke a robust immune response. Conversely, inactivated vaccines like Sinovac’s CoronaVac, which contain killed pathogens, generally produce fewer systemic side effects but may require multiple doses (e.g., two doses spaced 2–4 weeks apart) to achieve adequate immunity. This trade-off highlights the importance of balancing efficacy and tolerability when selecting a vaccine.
Practical tips for managing side effects vary by vaccine type. For mRNA vaccines, over-the-counter pain relievers like acetaminophen or ibuprofen can alleviate discomfort, but these should be taken only if symptoms arise, not preemptively. For viral vector vaccines, individuals should seek immediate medical attention if they experience severe headaches, abdominal pain, or unusual bruising within three weeks of vaccination, as these could indicate TTS. Pregnant individuals and those with a history of blood disorders should consult healthcare providers before receiving viral vector vaccines, as their risk profiles differ.
Comparatively, protein subunit vaccines like Novavax, which use harmless pieces of the virus, offer a middle ground in terms of side effects. Clinical trials showed that while recipients experienced injection site pain and fatigue, severe reactions were rare. This makes subunit vaccines a promising option for individuals hesitant about mRNA or viral vector vaccines. However, their availability and distribution vary globally, limiting access in some regions.
In conclusion, each vaccine’s side effect profile is a reflection of its design and mechanism. By understanding these differences, individuals can make informed choices and prepare for potential reactions. Healthcare providers play a critical role in educating patients about what to expect and how to respond, ensuring that the benefits of vaccination far outweigh the risks.
Crafting a Dinosaur Piggy Bank: A Fun DIY Project for Kids
You may want to see also
Frequently asked questions
mRNA vaccines use genetic material (messenger RNA) to instruct cells to produce a harmless piece of the COVID-19 virus spike protein, triggering an immune response. Viral vector vaccines, on the other hand, use a modified, harmless virus (vector) to deliver genetic instructions to cells to produce the spike protein, prompting immunity.
Inactivated vaccines contain a killed version of the COVID-19 virus, which cannot cause disease but still triggers an immune response. Unlike mRNA or viral vector vaccines, they do not use genetic material and typically require multiple doses and an adjuvant to enhance immunity.
Single-dose vaccines, such as Johnson & Johnson, are designed to provide sufficient immunity with just one shot, while multi-dose vaccines, like Pfizer-BioNTech and Moderna, require two or more doses spaced weeks apart to achieve full protection.
Protein subunit vaccines contain harmless pieces of the COVID-19 virus (e.g., the spike protein) made in a lab, which stimulate an immune response. Unlike mRNA or viral vector vaccines, they do not use genetic material and often include an adjuvant to boost the immune response.
Vaccines from different countries vary in their technology, efficacy rates, and regulatory approvals. For example, Pfizer-BioNTech uses mRNA technology and has high efficacy against symptomatic COVID-19, while Sinopharm uses inactivated virus technology and has varying efficacy rates based on studies. Regulatory standards and availability also differ by region.