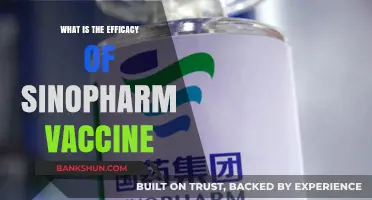
The efficacy of different vaccines varies significantly depending on the disease they target, the vaccine’s mechanism of action, and the population being vaccinated. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna have demonstrated high efficacy rates of around 94-95% against symptomatic COVID-19, while viral vector vaccines such as AstraZeneca and Johnson & Johnson show slightly lower efficacy, ranging from 67-90%. Similarly, traditional vaccines like the measles, mumps, and rubella (MMR) vaccine boast efficacy rates exceeding 97%, making them highly effective in preventing these diseases. Factors such as age, immune status, and the prevalence of circulating virus variants also influence vaccine efficacy, highlighting the importance of ongoing research and tailored vaccination strategies to optimize protection across diverse populations.
Vaccine Efficacy Comparison
| Characteristics | Values |
|---|---|
| Vaccine | Efficacy Against Symptomatic Infection |
| Pfizer-BioNTech (mRNA) | 95% (original strain), 67-75% (Delta), 40-50% (Omicron BA.1/BA.2) |
| Moderna (mRNA) | 94.1% (original strain), 75-80% (Delta), 40-50% (Omicron BA.1/BA.2) |
| Oxford-AstraZeneca (Viral Vector) | 70-82% (original strain), 60-70% (Delta), 30-40% (Omicron BA.1/BA.2) |
| Johnson & Johnson (Viral Vector) | 66% (original strain), 60-70% (Delta), 30-40% (Omicron BA.1/BA.2) |
| Sinopharm (Inactivated Virus) | 78-86% (original strain), 50-60% (Delta), 20-30% (Omicron BA.1/BA.2) |
| Sinovac (Inactivated Virus) | 50-84% (original strain, depending on study), 40-50% (Delta), 20-30% (Omicron BA.1/BA.2) |
| Novavax (Protein Subunit) | 90.4% (original strain), 70-80% (Delta), 40-50% (Omicron BA.1/BA.2) |
| Notes: | Efficacy rates vary based on strain, time since vaccination, and study methodology. These values are approximate and may change as more data becomes available. |
Explore related products






What You'll Learn
- COVID-19 Vaccines: Comparative effectiveness of mRNA, viral vector, and protein subunit vaccines
- Influenza Vaccines: Efficacy of seasonal vs. universal flu vaccines in diverse populations
- Childhood Vaccines: Impact of MMR, DTaP, and polio vaccines on disease prevention
- HPV Vaccines: Protection against cervical cancer and other HPV-related diseases
- Malaria Vaccines: Current efficacy of RTS,S and other malaria vaccine candidates
![]()
COVID-19 Vaccines: Comparative effectiveness of mRNA, viral vector, and protein subunit vaccines
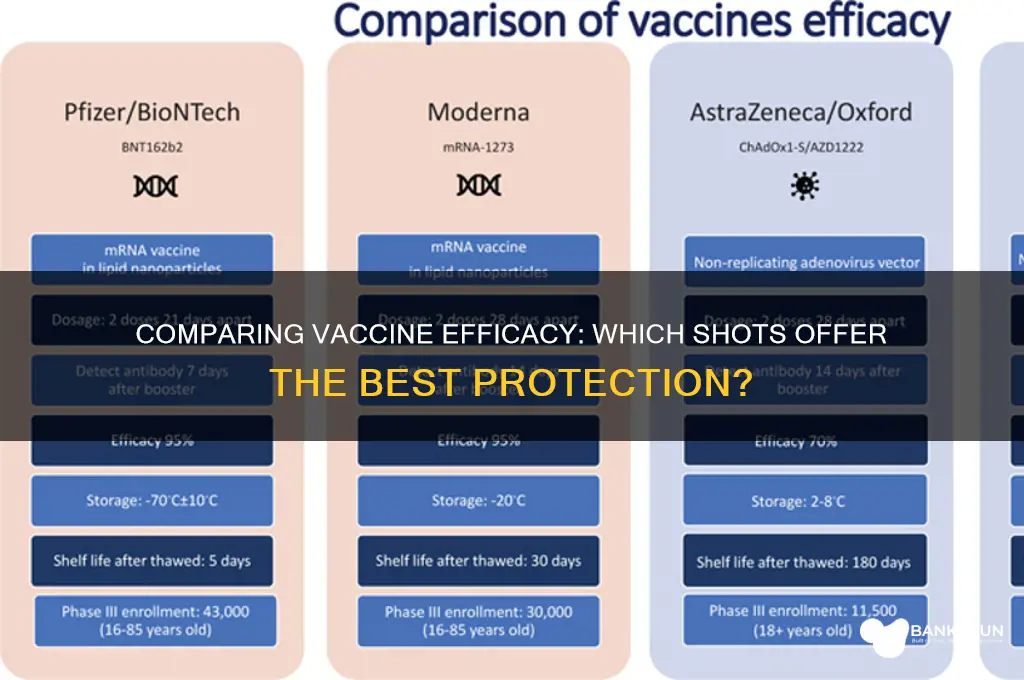
The COVID-19 pandemic spurred an unprecedented global effort to develop vaccines, resulting in three primary technologies: mRNA, viral vector, and protein subunit vaccines. Each platform demonstrated unique efficacy profiles, influenced by factors like dosage, age, and emerging variants. Understanding these differences is crucial for informed decision-making, especially as booster strategies evolve.
MRNA Vaccines: Pfizer-BioNTech and Moderna
MRNA vaccines, exemplified by Pfizer-BioNTech (BNT162b2) and Moderna (mRNA-1273), emerged as frontrunners with initial efficacy rates of 95% and 94.1%, respectively, against symptomatic COVID-19 in clinical trials. These vaccines require a two-dose regimen, typically administered 3–4 weeks apart, with a 30-microgram dose for Pfizer and a 100-microgram dose for Moderna. Their high efficacy is attributed to robust neutralizing antibody production and T-cell responses. However, real-world data show waning immunity over 6–12 months, particularly against variants like Delta and Omicron. Boosters restore protection, with a 20–30 percentage point increase in efficacy against symptomatic infection. These vaccines are approved for individuals aged 5 and older, with dosage adjustments for younger age groups (e.g., 10 micrograms for children 5–11).
Viral Vector Vaccines: AstraZeneca and Johnson & Johnson
Viral vector vaccines, such as AstraZeneca (ChAdOx1 nCoV-19) and Johnson & Johnson (Ad26.COV2.S), utilize modified adenoviruses to deliver genetic material. AstraZeneca’s efficacy ranges from 62% to 90%, depending on dosing intervals, with a two-dose regimen 8–12 weeks apart. Johnson & Johnson’s single-dose vaccine offers 66%–72% efficacy against symptomatic disease. While lower than mRNA vaccines, these options provide strong protection against severe illness and hospitalization, particularly in resource-limited settings. However, rare side effects like thrombosis with thrombocytopenia syndrome (TTS) have limited their use in certain demographics. These vaccines are typically recommended for adults aged 18 and older, with Johnson & Johnson often used in hard-to-reach populations due to its single-dose convenience.
Protein Subunit Vaccines: Novavax
Novavax’s NVX-CoV2373, a protein subunit vaccine, offers a distinct approach by delivering stabilized spike proteins with an adjuvant to enhance immune response. Clinical trials reported 90.4% efficacy against symptomatic COVID-19, with a two-dose regimen administered 3 weeks apart. This vaccine is particularly appealing for individuals hesitant about newer technologies, as it relies on traditional vaccine methods. Novavax has shown effectiveness against variants like Alpha and Delta, though data on Omicron are still emerging. Approved for adults aged 18 and older, it provides a valuable alternative for those with mRNA or viral vector contraindications.
Comparative Takeaways and Practical Tips
While mRNA vaccines lead in initial efficacy and booster response, viral vector and protein subunit vaccines offer robust protection against severe disease and hospitalization. When choosing a vaccine, consider factors like age, comorbidities, and local variant prevalence. For optimal protection, adhere to recommended dosing intervals and stay updated on booster guidelines. Pregnant individuals and those with specific allergies should consult healthcare providers for tailored advice. Regardless of the platform, vaccination remains the most effective tool in reducing COVID-19 morbidity and mortality.
Are FirstRand Bank and FNB the Same? Unraveling the Connection
You may want to see also
Explore related products


$16.86 $16.95




![]()
Influenza Vaccines: Efficacy of seasonal vs. universal flu vaccines in diverse populations
Influenza vaccines are a cornerstone of public health, yet their efficacy varies widely depending on the type of vaccine and the population receiving it. Seasonal flu vaccines, updated annually to match circulating strains, typically offer 40–60% protection in healthy adults. However, this efficacy drops significantly in older adults and immunocompromised individuals due to age-related immune decline and underlying health conditions. For instance, in those over 65, efficacy often hovers around 20–30%, prompting the development of high-dose formulations like Fluzone High-Dose, which contain 4x the standard antigen (120 µg vs. 30 µg) to enhance immune response. In contrast, universal flu vaccines aim to target conserved viral proteins, offering broader, longer-lasting protection across multiple strains. While still in clinical trials, early data suggest these vaccines could provide 60–70% efficacy across diverse populations, including vulnerable groups, by focusing on the stalk of the hemagglutinin protein rather than its strain-specific head.
Consider the logistical challenges of these two approaches. Seasonal vaccines require global surveillance, strain selection, and annual production, a process that can lead to mismatches if circulating strains evolve unexpectedly. This was evident in the 2014–2015 season, when vaccine efficacy plummeted to 19% due to a H3N2 variant. Universal vaccines, however, could eliminate the need for yearly updates, reducing production complexity and ensuring consistent protection. For example, a universal vaccine candidate like M-001, currently in Phase II trials, has shown promise in eliciting robust T-cell responses in both young and elderly populations, potentially offering a one-size-fits-all solution. However, their success hinges on overcoming technical hurdles, such as ensuring sufficient immunogenicity without adverse effects, and securing regulatory approval.
A critical factor in vaccine efficacy is population diversity, encompassing age, ethnicity, and geographic location. Seasonal vaccines often underperform in low-resource settings due to limited access and storage challenges, while universal vaccines could bridge this gap by providing stable, long-lasting immunity. For instance, in sub-Saharan Africa, where influenza surveillance is limited, a universal vaccine could offer consistent protection against both seasonal and pandemic strains. Additionally, certain ethnic groups, such as Indigenous populations, experience higher flu-related hospitalizations, highlighting the need for vaccines tailored to diverse immune profiles. Studies show that adjuvanted vaccines, like MF59-containing formulations, improve efficacy in these groups by enhancing immune responses, though their availability remains limited.
Practical considerations for healthcare providers include optimizing vaccine delivery to maximize efficacy. For seasonal vaccines, administering high-dose or adjuvanted formulations to older adults and immunocompromised patients can significantly improve outcomes. For example, the CDC recommends Fluad, an MF59-adjuvanted vaccine, for those over 65 due to its 25% higher efficacy compared to standard-dose vaccines. For universal vaccines, once approved, prioritizing at-risk populations during initial rollout will be crucial. Providers should also educate patients about the limitations of current vaccines and the potential benefits of universal alternatives, fostering informed decision-making.
In conclusion, while seasonal flu vaccines remain the current standard, their variable efficacy underscores the need for innovation. Universal vaccines, though still experimental, hold transformative potential by offering consistent protection across diverse populations. Until then, healthcare systems must leverage existing tools, such as high-dose and adjuvanted vaccines, to address disparities in efficacy. By combining targeted strategies with advancements in vaccine technology, we can move closer to a future where influenza is no longer a seasonal threat but a manageable, preventable illness.
Banks as Tenants: A Good Lease Deal?
You may want to see also
Explore related products

$18.59 $19.95

$22.99




![]()
Childhood Vaccines: Impact of MMR, DTaP, and polio vaccines on disease prevention
Childhood vaccines have been a cornerstone of public health, dramatically reducing the incidence of once-devastating diseases. Among these, the MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), and polio vaccines stand out for their profound impact on disease prevention. The MMR vaccine, typically administered in two doses—the first at 12-15 months and the second at 4-6 years—has achieved a 97% efficacy rate against measles after two doses. This has led to a 99% reduction in measles cases globally since the vaccine’s introduction in 1963. Similarly, the DTaP vaccine, given in a series of five shots starting at 2 months of age, provides 80-85% protection against pertussis (whooping cough) in the first year after completion, significantly curbing outbreaks in young children. Polio vaccines, both the inactivated poliovirus vaccine (IPV) and the oral poliovirus vaccine (OPV), have been instrumental in eradicating polio in all but two countries, with IPV offering 99% protection after three doses.
Analyzing the efficacy of these vaccines reveals their unique contributions to disease prevention. The MMR vaccine not only protects against individual diseases but also prevents complications like pneumonia, encephalitis, and congenital rubella syndrome. For instance, rubella vaccination has eliminated congenital rubella syndrome in over 80 countries. The DTaP vaccine’s effectiveness wanes over time, necessitating booster shots (DT or Tdap) for adolescents and adults to maintain immunity. Polio vaccines have a dual role: IPV provides individual protection, while OPV induces intestinal immunity, reducing viral transmission in communities. This combination has been critical in the global polio eradication initiative.
Practical implementation of these vaccines requires adherence to specific guidelines. For the MMR vaccine, ensuring timely administration of both doses is crucial, as even a small delay can leave children vulnerable during outbreaks. Parents should be aware that mild side effects, such as fever or rash, are common but far less severe than the diseases themselves. The DTaP vaccine series must be completed on schedule (at 2, 4, 6, 15-18 months, and 4-6 years) to maximize protection, especially against pertussis, which remains a threat to infants too young to be fully vaccinated. Polio vaccination strategies vary by region: in polio-free countries, IPV is the standard, while OPV is used in outbreak response to rapidly interrupt transmission.
Comparing these vaccines highlights their collective role in shaping global health. While the MMR vaccine’s high efficacy has nearly eliminated measles in many regions, ongoing vaccination is essential to prevent resurgence, as seen in recent outbreaks linked to vaccine hesitancy. The DTaP vaccine’s moderate efficacy against pertussis underscores the importance of herd immunity, as vaccinated individuals reduce disease spread even if they are not fully protected. Polio vaccines exemplify the power of global collaboration, with coordinated efforts bringing the world to the brink of eradication. Together, these vaccines demonstrate how targeted immunization can transform disease landscapes.
In conclusion, the MMR, DTaP, and polio vaccines are pillars of childhood immunization, each with distinct mechanisms and impacts. Their efficacy rates, while impressive, rely on consistent administration and global cooperation. Parents and healthcare providers must remain vigilant, ensuring children receive vaccines on schedule and addressing misinformation that threatens progress. By understanding the unique contributions of these vaccines, we can sustain their success and protect future generations from preventable diseases.
Activate Andhra Bank Safe T: A Step-by-Step Guide for Secure Banking
You may want to see also
Explore related products






![]()
HPV Vaccines: Protection against cervical cancer and other HPV-related diseases
Human papillomavirus (HPV) vaccines stand as a cornerstone in the prevention of cervical cancer and other HPV-related diseases, offering remarkable efficacy in reducing infection rates and associated health risks. Clinical trials have consistently shown that HPV vaccines, such as Gardasil 9, provide nearly 100% protection against the high-risk HPV types (16, 18, 31, 33, 45, 52, 58) responsible for approximately 90% of cervical cancers. This protection extends to other cancers, including anal, oropharyngeal, and vulvar cancers, as well as genital warts caused by low-risk HPV types (6, 11). The vaccine’s efficacy is highest when administered before potential exposure to the virus, underscoring the importance of early vaccination.
The recommended HPV vaccination schedule typically involves two doses for individuals aged 9 to 14, with a minimum interval of six months between doses. For those aged 15 to 26, a three-dose series is advised, administered at 0, 1–2, and 6 months. While the vaccine is most effective in pre-teens and adolescents, it is also approved for adults up to age 45, though its benefits are more limited due to prior exposure to HPV. Adhering to the dosing schedule is critical, as incomplete vaccination reduces efficacy. Parents and healthcare providers should prioritize timely administration to maximize protection, particularly for young adolescents before they become sexually active.
A comparative analysis of HPV vaccines reveals their superiority over other preventive measures for cervical cancer. Unlike Pap smears, which detect precancerous changes, HPV vaccines prevent infection altogether, offering a proactive rather than reactive approach. Moreover, the vaccines’ efficacy surpasses that of many other vaccines, such as the influenza vaccine, which varies annually based on strain matching. HPV vaccines’ consistent high efficacy across diverse populations highlights their role as a public health triumph, significantly reducing the global burden of HPV-related diseases.
Despite their proven efficacy, HPV vaccines face challenges in uptake due to misconceptions and hesitancy. Addressing these barriers requires education on the vaccine’s safety and long-term benefits. Practical tips for improving vaccination rates include integrating HPV vaccination into routine adolescent immunizations, offering school-based vaccination programs, and leveraging healthcare provider recommendations. Additionally, emphasizing that the vaccine protects against multiple cancers and diseases, not just cervical cancer, can broaden its appeal. By dispelling myths and promoting accessibility, societies can fully harness the potential of HPV vaccines to save lives.
In conclusion, HPV vaccines represent a groundbreaking tool in the fight against cervical cancer and other HPV-related diseases, with efficacy rates that rival or exceed those of many other vaccines. Their ability to prevent infection before it occurs underscores their value as a primary prevention strategy. By following recommended dosing schedules, targeting vaccination efforts at younger age groups, and addressing barriers to uptake, communities can maximize the impact of HPV vaccines. This proactive approach not only reduces individual health risks but also contributes to global efforts to eliminate cervical cancer as a public health threat.
Is the Bank of Dave a Real Deal or Just a Myth?
You may want to see also
Explore related products






![]()
Malaria Vaccines: Current efficacy of RTS,S and other malaria vaccine candidates
Malaria remains a significant global health challenge, with approximately 247 million cases and 619,000 deaths reported in 2021, primarily in children under five in sub-Saharan Africa. The development of an effective malaria vaccine has been a long-standing goal, and RTS,S, the first and only approved malaria vaccine, marks a pivotal step forward. Developed by GSK in partnership with the Malaria Vaccine Initiative, RTS,S targets the *Plasmodium falciparum* parasite, the deadliest malaria-causing pathogen. Clinical trials have shown that RTS,S provides moderate efficacy, reducing severe malaria cases by about 30% in children aged 5–17 months who received a 4-dose regimen. While this efficacy is lower than many other vaccines, such as the 95% efficacy of the Pfizer-BioNTech COVID-19 vaccine, it still represents a critical tool in malaria control when combined with other interventions like bed nets and antimalarial drugs.
The RTS,S vaccine’s efficacy wanes over time, necessitating a booster dose to maintain protection. A phase 3 trial demonstrated that a fourth dose administered 18 months after the initial series restored efficacy to levels comparable to the primary series. However, the vaccine’s rollout has been limited by logistical challenges, including the need for a cold chain and the complexity of the dosing schedule. Despite these limitations, the World Health Organization (WHO) endorsed RTS,S in 2021 for use in children in moderate-to-high malaria transmission areas, highlighting its potential to save tens of thousands of lives annually. Practical implementation requires careful planning, such as integrating vaccination campaigns with routine immunization programs and ensuring community engagement to improve uptake.
Beyond RTS,S, several other malaria vaccine candidates are in advanced stages of development, each with unique mechanisms and efficacy profiles. The R21/Matrix-M vaccine, developed by the University of Oxford, has shown promising results in phase 2b trials, with 77% efficacy in children aged 5–17 months after a 3-dose regimen. This vaccine uses a similar recombinant protein approach to RTS,S but includes an adjuvant to enhance immune response. Another candidate, the whole-parasite vaccine PfSPZ, developed by Sanaria, uses radiation-attenuated sporozoites and has demonstrated up to 100% protection in small-scale trials, though its efficacy decreases with higher parasite exposure. These candidates offer hope for higher and more durable protection but face challenges in scalability and cost-effectiveness.
Comparing these vaccines reveals trade-offs between efficacy, practicality, and accessibility. RTS,S, despite its moderate efficacy, has the advantage of being the only approved vaccine with an established supply chain. R21/Matrix-M, while more efficacious, is still awaiting regulatory approval and large-scale manufacturing validation. PfSPZ, though highly effective, requires intravenous administration, making it less suitable for mass vaccination campaigns. For public health officials, the choice of vaccine will depend on local malaria burden, healthcare infrastructure, and cost considerations. For instance, in regions with high transmission, a vaccine with even moderate efficacy, like RTS,S, could significantly reduce mortality when combined with other interventions.
To maximize the impact of malaria vaccines, a multi-pronged strategy is essential. This includes optimizing vaccine delivery through integrated health systems, ensuring equitable access, and continuing research to improve efficacy and durability. For parents and caregivers in endemic areas, staying informed about vaccine availability and adhering to recommended schedules is crucial. Additionally, combining vaccination with preventive measures like insecticide-treated bed nets and prompt treatment of malaria cases can amplify protection. While no single vaccine will eliminate malaria, the current and emerging candidates represent vital tools in the fight against this devastating disease.
Local Food Banks: Empowering Communities to Fight Poverty Effectively
You may want to see also
Frequently asked questions
The Pfizer-BioNTech COVID-19 vaccine has demonstrated an efficacy of approximately 95% in preventing symptomatic COVID-19 infection in clinical trials, based on two doses administered 21 days apart.
The Moderna COVID-19 vaccine has shown an efficacy of around 94.1% in preventing symptomatic COVID-19 in clinical trials, similar to Pfizer-BioNTech, with two doses given 28 days apart.
The Johnson & Johnson COVID-19 vaccine has an efficacy of about 66% in preventing moderate to severe COVID-19 globally, and higher efficacy (around 72%) in the United States, based on a single dose.
Flu vaccine efficacy varies annually, typically ranging between 40% and 60%, depending on the match between the vaccine strains and circulating flu viruses. It remains the best defense against severe flu illness.