The H1N1 vaccine, developed to combat the influenza A (H1N1) virus, commonly known as swine flu, is composed of several key components designed to stimulate the immune system without causing the disease. The primary ingredient is the inactivated or weakened form of the H1N1 virus itself, which serves as the antigen to trigger an immune response. Depending on the specific formulation, the vaccine may also contain adjuvants, such as aluminum salts, to enhance the body’s immune reaction. Additionally, stabilizers like gelatin or sugars are included to maintain the vaccine’s effectiveness during storage. Some versions may also contain preservatives, such as thimerosal, to prevent contamination, though many modern vaccines are preservative-free. The exact composition can vary between manufacturers and vaccine types, such as inactivated (injectable) or live attenuated (nasal spray) formulations, but all are rigorously tested for safety and efficacy before approval.
Explore related products






What You'll Learn
- Vaccine Components: Includes antigens, adjuvants, preservatives, stabilizers, and residual manufacturing materials in small amounts
- Antigen Source: Derived from inactivated or weakened H1N1 influenza virus strains
- Adjuvants Role: Enhance immune response, often using oils or aluminum salts in formulation
- Preservatives Used: Thimerosal or similar agents prevent bacterial contamination in multi-dose vials
- Manufacturing Process: Grown in eggs or cell cultures, then purified and tested for safety
![]()
Vaccine Components: Includes antigens, adjuvants, preservatives, stabilizers, and residual manufacturing materials in small amounts
The H1N1 vaccine, like many vaccines, is a complex formulation designed to trigger a protective immune response without causing the disease itself. At its core are antigens, specifically inactivated or weakened fragments of the H1N1 influenza virus. These antigens are the key players, teaching the immune system to recognize and combat the virus if exposed in the future. For instance, the 2009 H1N1 pandemic vaccine contained 15 micrograms of hemagglutinin, a surface protein of the virus, per dose—a precise amount calibrated to ensure efficacy without overwhelming the body.
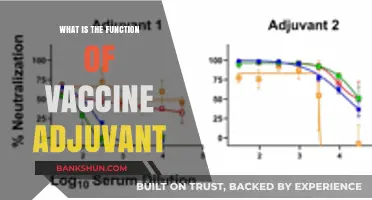
Beyond antigens, adjuvants are often included to enhance the immune response, particularly in vaccines with lower antigen doses. Adjuvants like aluminum salts (e.g., aluminum hydroxide) act by creating a depot effect, slowly releasing the antigen to prolong immune system exposure. This is especially useful in pandemic scenarios where rapid, large-scale vaccine production is necessary, and adjuvants can stretch limited antigen supplies. For example, the AS03 adjuvant system was used in some H1N1 vaccines, allowing for a lower antigen dose while maintaining robust immunity.
Preservatives and stabilizers are critical for ensuring vaccine safety and longevity. Preservatives like thimerosal, used in multi-dose vials, prevent bacterial or fungal contamination, though single-dose vials often omit these to cater to preservative-sensitive populations. Stabilizers such as sugars (e.g., sucrose or lactose) protect the vaccine’s components from degradation during storage and transport, particularly important for vaccines distributed globally under varying environmental conditions.
Finally, residual manufacturing materials are present in trace amounts, a byproduct of the production process. These include antibiotics (e.g., neomycin or gentamicin) used to prevent bacterial growth during manufacturing, and inorganic compounds like formaldehyde, which inactivates viruses during production. Regulatory agencies strictly limit these residues to levels far below those known to cause harm, ensuring safety across age groups, from children to the elderly.
Understanding these components demystifies the H1N1 vaccine’s composition, highlighting the balance between efficacy, safety, and practicality. For instance, parents concerned about adjuvants or preservatives can opt for single-dose, preservative-free formulations, while healthcare providers can educate patients about the purpose of each ingredient, fostering trust in vaccination programs. This transparency is crucial, especially in addressing vaccine hesitancy fueled by misinformation.
WSU Disbursement to Bank Timeline: What to Expect
You may want to see also
Explore related products






![]()
Antigen Source: Derived from inactivated or weakened H1N1 influenza virus strains
The H1N1 vaccine's core component is its antigen source, derived from inactivated or weakened strains of the H1N1 influenza virus. This approach ensures the vaccine stimulates an immune response without causing the disease itself. Inactivated vaccines, such as the flu shot, use virus particles that have been killed, rendering them unable to replicate but still recognizable by the immune system. Weakened (attenuated) vaccines, like the nasal spray FluMist, use live viruses that are modified to be less virulent, suitable for healthy individuals aged 2 to 49. Both methods aim to prepare the body to fight off future H1N1 infections effectively.
Inactivated H1N1 vaccines are produced by growing the virus in chicken eggs or cell cultures, then chemically deactivating it. This process preserves the virus’s surface proteins, including hemagglutinin, which the immune system targets. A standard dose contains 15 micrograms of hemagglutinin antigen, administered via intramuscular injection, typically in the upper arm. This formulation is ideal for individuals with weakened immune systems, pregnant women, and those aged 65 and older, as it minimizes risks while providing robust protection.
Weakened H1N1 vaccines, on the other hand, are created by adapting the virus to grow at cooler temperatures, reducing its ability to cause illness in warmer parts of the body, like the lungs. The nasal spray delivers a lower antigen dose (approximately 10^6.5–7.5 flu virus particles) directly to the mucosal lining of the nose, mimicking natural infection and triggering a strong local immune response. This method is particularly effective for children and young adults, who often benefit from the added mucosal immunity. However, it is contraindicated for those with asthma, immunocompromised individuals, and pregnant women due to potential risks.
Choosing between inactivated and weakened vaccines depends on factors like age, health status, and personal preference. For instance, a 30-year-old with no chronic conditions might opt for the nasal spray for its convenience and broader immune response, while a 70-year-old with diabetes would likely benefit more from the inactivated injectable vaccine. Always consult a healthcare provider to determine the most suitable option, as individual medical history plays a critical role in vaccine selection.
Practical tips for vaccination include scheduling the shot or spray during the early fall, as flu season typically peaks in winter. After receiving the vaccine, monitor for mild side effects like soreness at the injection site, low-grade fever, or nasal congestion, which usually resolve within 1–2 days. Keep hydrated and rest if needed. For parents administering the nasal spray to children, ensure the child is upright and calm during application to avoid choking. By understanding the antigen source and its implications, individuals can make informed decisions to protect themselves and their communities from H1N1 influenza.
Evaluating the Reliability of Test Banks Solution Zone: A Comprehensive Review
You may want to see also
Explore related products






![]()
Adjuvants Role: Enhance immune response, often using oils or aluminum salts in formulation
Adjuvants are the unsung heroes of vaccine formulation, playing a critical role in amplifying the immune response to antigens. In the context of the H1N1 vaccine, adjuvants such as oils (e.g., squalene-based MF59) or aluminum salts (e.g., aluminum hydroxide) are often incorporated to ensure the body mounts a robust defense against the influenza virus. These substances act as immune system accelerators, reducing the amount of antigen needed while prolonging its release, which is particularly crucial for rapid vaccine production during pandemics. For instance, the AS03 adjuvant system, used in some H1N1 vaccines, contains DL-α-tocopherol (vitamin E) and squalene, enhancing immunity even with lower antigen doses.
Consider the practical implications of adjuvant use: aluminum salts, commonly used in vaccines for decades, are generally well-tolerated but can cause localized reactions like redness or swelling at the injection site. Oil-in-water emulsions, on the other hand, may induce stronger systemic responses, such as mild fever or fatigue, but these are typically short-lived. For children and the elderly, adjuvanted vaccines often provide better protection due to their ability to stimulate a more vigorous immune response, even in immunocompromised individuals. However, dosage adjustments are critical; for example, the AS03 adjuvant is typically used in a 0.5 mL dose for adults, while children may receive a lower volume to minimize side effects.
From a comparative standpoint, adjuvants like MF59 and aluminum salts differ in their mechanisms of action. Aluminum salts primarily act as antigen depots, slowing release and prolonging exposure to the immune system. In contrast, oil-based adjuvants create a local inflammatory response, recruiting immune cells to the injection site. This distinction is vital when formulating vaccines for different populations. For instance, pregnant women, who are at higher risk for severe H1N1 complications, may benefit from adjuvanted vaccines but require careful monitoring due to potential fetal exposure to adjuvant components.
To maximize the benefits of adjuvanted H1N1 vaccines, follow these practical tips: administer the vaccine intramuscularly, as this route optimizes adjuvant activity. Store vaccines containing oil-based adjuvants at 2–8°C to maintain emulsion stability, and avoid freezing. Educate recipients about potential side effects, emphasizing that transient reactions like soreness or fatigue are normal and indicate immune activation. Finally, for individuals with a history of severe allergic reactions to adjuvant components, consult an allergist before vaccination to assess risks and explore alternative formulations.
In conclusion, adjuvants are not mere additives but strategic components that elevate the efficacy of H1N1 vaccines. By understanding their role, mechanisms, and practical considerations, healthcare providers can optimize vaccine administration and ensure broader protection against influenza. Whether using aluminum salts or oil-based systems, the goal remains the same: to harness the immune system’s full potential in the fight against H1N1.
Understanding Islamic Banking: Core Principles and Practices Explained
You may want to see also
Explore related products






![]()
Preservatives Used: Thimerosal or similar agents prevent bacterial contamination in multi-dose vials
Multi-dose vials of the H1N1 vaccine often contain preservatives like thimerosal to prevent bacterial contamination. This mercury-based compound acts as a safeguard, ensuring the vaccine remains sterile and safe for use, even after repeated needle punctures. Thimerosal breaks down into ethylmercury in the body, which is rapidly eliminated, unlike its more toxic counterpart, methylmercury. The U.S. Centers for Disease Control and Prevention (CDC) notes that the amount of thimerosal in vaccines is minimal—typically 25 micrograms per dose—and well below levels considered harmful. This preservative has been used for decades in various vaccines, with no scientific evidence linking it to adverse health effects.
While thimerosal is effective, its inclusion in vaccines has sparked controversy, particularly among those concerned about mercury exposure. However, it’s crucial to distinguish between ethylmercury and methylmercury. Ethylmercury, found in thimerosal, does not accumulate in the body and is excreted quickly, whereas methylmercury, found in certain fish, can build up and cause toxicity. For context, a single dose of thimerosal-preserved vaccine contains less ethylmercury than a 3-ounce can of tuna. Despite this, some vaccine manufacturers offer thimerosal-free versions, particularly for pediatric doses, to address public concerns and provide options for those who prefer preservative-free formulations.
The use of thimerosal is not limited to the H1N1 vaccine; it’s also found in other multi-dose influenza vaccines. This is particularly important in settings where vaccine supply is limited or where frequent access to single-dose vials is impractical. For instance, in mass vaccination campaigns during a pandemic, multi-dose vials with thimerosal allow healthcare providers to administer the vaccine efficiently to large populations. The World Health Organization (WHO) supports the use of thimerosal in vaccines, emphasizing its safety profile and its role in preventing contamination that could lead to serious infections.
If you’re concerned about thimerosal, discuss your options with a healthcare provider. Pregnant women, infants, and young children are often prioritized for thimerosal-free formulations, though the preserved versions remain safe for all age groups. It’s also worth noting that not all vaccines contain thimerosal—single-dose vials are typically preservative-free. Always verify the vaccine type and its components before administration, especially if you have specific health concerns or allergies. Understanding the role of preservatives like thimerosal can help you make informed decisions about vaccination, ensuring both safety and efficacy.
Revitalize Your Immune System Post-Vaccination: A Comprehensive Reset Guide
You may want to see also
Explore related products






![]()
Manufacturing Process: Grown in eggs or cell cultures, then purified and tested for safety
The H1N1 vaccine, like many influenza vaccines, begins its journey in a biological incubator—either eggs or cell cultures. This foundational step is crucial because the virus needs a living host to replicate. Historically, chicken eggs have been the go-to medium, a method dating back to the 1940s. Each egg is inoculated with a strain of the H1N1 virus, which then multiplies inside the embryo over several days. Alternatively, modern manufacturing uses cell cultures, often derived from mammalian cells, which offer a faster and more scalable process. This shift is particularly important for individuals with egg allergies, as cell-based vaccines eliminate the risk of allergic reactions.
Once the virus has sufficiently replicated, the next phase involves purification. The raw material—whether from eggs or cell cultures—contains not only the virus but also proteins, DNA, and other cellular debris. To isolate the viral particles, manufacturers use a series of filtration and chemical processes. One common technique is centrifugation, which separates the virus from larger impurities. This is followed by treatment with detergents or enzymes to break down unwanted materials. The result is a concentrated viral solution, ready for the next step: inactivation or attenuation. Inactivated vaccines, like most H1N1 vaccines, are treated with chemicals such as formaldehyde to render the virus non-infectious while preserving its ability to trigger an immune response.
Safety testing is the final and most critical stage before distribution. Each batch of the H1N1 vaccine undergoes rigorous evaluation to ensure it meets regulatory standards. This includes sterility tests to confirm the absence of bacterial or fungal contamination, potency assays to verify the vaccine’s effectiveness, and stability checks to ensure it remains viable throughout its shelf life. For example, the U.S. Food and Drug Administration (FDA) requires manufacturers to demonstrate that the vaccine contains the correct antigen concentration, typically measured in micrograms per dose. A standard dose for adults is 15 micrograms of hemagglutinin, the key protein that elicits an immune response. Pediatric doses may be lower, depending on the child’s age—for instance, 7.5 micrograms for children aged 6 months to 3 years.
Practical considerations for healthcare providers and recipients are equally important. The vaccine is typically administered as a single intramuscular injection, usually in the deltoid muscle for adults and the anterolateral thigh for infants. Side effects are generally mild and may include soreness at the injection site, low-grade fever, or fatigue. These symptoms usually resolve within 48 hours. For optimal protection, vaccination is recommended annually, as the circulating H1N1 strains can evolve. Pregnant women, the elderly, and individuals with chronic conditions are prioritized due to their higher risk of complications from influenza. By understanding the manufacturing process—from egg or cell culture to purification and testing—both providers and the public can appreciate the science behind this life-saving intervention.
Essential Vaccines for Kids: Full Immunization Guide by Age 6
You may want to see also
Frequently asked questions
The H1N1 vaccine primarily contains inactivated (killed) H1N1 virus strains, adjuvants (to enhance immune response), stabilizers, and preservatives (like thimerosal in some formulations).
No, the H1N1 vaccine contains inactivated (killed) virus, making it impossible to contract the flu from the vaccine.
Some H1N1 vaccines may contain trace amounts of antibiotics (e.g., neomycin) used during production, and the virus is often grown in chicken eggs, so egg proteins may be present in small quantities.
Some multi-dose vials of the H1N1 vaccine contain thimerosal as a preservative, but single-dose vials are typically thimerosal-free.
No, the H1N1 vaccine is not an mRNA vaccine. It uses traditional technology with inactivated virus particles, unlike mRNA vaccines like those for COVID-19.