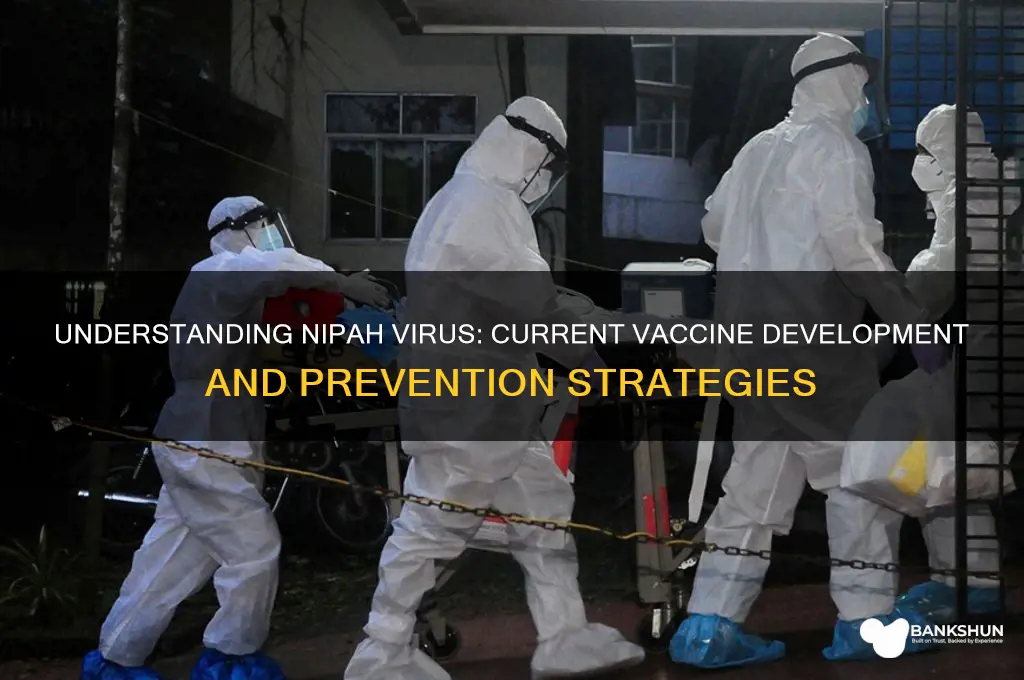
The Nipah virus, a zoonotic pathogen primarily transmitted from animals to humans, poses a significant public health threat due to its high mortality rate and potential for outbreaks. As of now, there is no commercially available vaccine for humans, though several candidates are under development. Research efforts have focused on creating vaccines that can effectively prevent infection, with some promising results in preclinical and early clinical trials. These include recombinant subunit vaccines, virus-like particle vaccines, and mRNA-based approaches. The urgency to develop a Nipah virus vaccine is heightened by the virus's ability to cause severe respiratory and neurological diseases, as well as its potential for person-to-person transmission. International collaborations and funding are crucial to accelerate vaccine development and ensure global preparedness against this deadly virus.
Explore related products

$16.99





What You'll Learn
- Vaccine Development Status: Current progress and challenges in creating a Nipah virus vaccine
- Vaccine Types: Overview of potential vaccine platforms (e.g., mRNA, viral vector)
- Clinical Trials: Updates on human testing phases and safety data
- Global Accessibility: Plans for distribution and affordability in affected regions
- Effectiveness: Expected efficacy against Nipah virus strains and duration of protection
![]()
Vaccine Development Status: Current progress and challenges in creating a Nipah virus vaccine
The Nipah virus, a zoonotic pathogen with a high mortality rate, has sparked urgent efforts to develop an effective vaccine. Despite its emergence over two decades ago, no licensed vaccine is yet available for human use. However, significant strides have been made in preclinical and clinical trials, offering a glimmer of hope in the fight against this deadly virus. Several vaccine candidates, including recombinant subunit vaccines, virus-like particles (VLPs), and live-attenuated vaccines, are under investigation, each with unique mechanisms and potential advantages.
One of the most promising candidates is the recombinant Nipah G glycoprotein vaccine, which has shown robust immune responses in animal models. This vaccine, developed using the Hendra virus G glycoprotein as a backbone, has advanced to Phase 1 clinical trials. Early results indicate its safety and immunogenicity in healthy adults, with doses ranging from 20 to 100 micrograms administered intramuscularly. If successful, this candidate could pave the way for a dual-purpose vaccine protecting against both Nipah and Hendra viruses, streamlining development and deployment efforts.
Despite these advancements, challenges persist. The Nipah virus’s sporadic outbreaks and limited geographic distribution complicate large-scale clinical trials, making it difficult to assess vaccine efficacy in real-world settings. Additionally, the virus’s ability to mutate poses a risk of vaccine escape, necessitating the development of broadly protective immunogens. Funding and prioritization also remain hurdles, as Nipah competes with other high-profile pathogens for resources. Public health officials must balance investment in Nipah vaccines with the immediate needs of more widespread diseases, a delicate calculus that slows progress.
Another critical challenge is ensuring equitable access to any eventual Nipah vaccine. Low- and middle-income countries, particularly in South and Southeast Asia, bear the brunt of Nipah outbreaks but often lack the infrastructure to distribute vaccines effectively. Strategies such as technology transfer, local manufacturing, and global partnerships will be essential to address this disparity. Practical steps, like training healthcare workers in vaccine administration and cold chain management, could significantly enhance preparedness in endemic regions.
In conclusion, while the journey toward a Nipah virus vaccine is fraught with obstacles, recent progress underscores the feasibility of this goal. From innovative vaccine designs to early clinical successes, the groundwork has been laid for a potential breakthrough. Addressing remaining challenges will require collaboration across scientific, financial, and logistical domains. For now, vigilance, research, and investment remain the cornerstones of turning the tide against Nipah.
UK's Global Vaccine Efforts: Understanding the Overseas Immunization Programme
You may want to see also
Explore related products





![]()
Vaccine Types: Overview of potential vaccine platforms (e.g., mRNA, viral vector)
The quest for a Nipah virus vaccine has spurred exploration of diverse vaccine platforms, each with unique mechanisms and potential advantages. Among these, mRNA and viral vector technologies have emerged as frontrunners, leveraging their proven efficacy in combating other pathogens like SARS-CoV-2. mRNA vaccines, such as those developed by Moderna and Pfizer-BioNTech, introduce genetic material encoding the Nipah virus’s glycoprotein, prompting the body to produce a harmless viral component that triggers an immune response. This platform offers rapid development and scalability, with potential for dose adjustments—typically a 30 µg dose for adults—and adaptability to viral mutations. Viral vector vaccines, exemplified by Oxford-AstraZeneca’s COVID-19 vaccine, use a modified virus (e.g., adenovirus) to deliver Nipah virus antigen genes. This approach benefits from established manufacturing processes and a single-dose regimen, though pre-existing immunity to the vector could limit efficacy in some populations.
Analyzing these platforms reveals trade-offs. mRNA vaccines boast high efficacy and rapid production but require ultra-cold storage, a challenge in resource-limited settings where Nipah outbreaks often occur. Viral vector vaccines, while more stable, may face reduced effectiveness in regions with high adenovirus prevalence. Both platforms, however, offer modularity, enabling swift responses to Nipah’s genetic diversity. For instance, a Nipah mRNA vaccine candidate could be redesigned within weeks if a new strain emerges, whereas viral vectors might require additional safety testing due to their reliance on live organisms.
Instructively, developing a Nipah vaccine demands consideration of target populations, such as healthcare workers and livestock handlers, who are at highest risk. mRNA vaccines could be tailored for adults with a two-dose regimen (28 days apart), while viral vector vaccines might prioritize single-dose convenience for rapid outbreak control. Practical tips include leveraging existing cold chain infrastructure for mRNA distribution and conducting seroprevalence studies to assess viral vector suitability in endemic regions.
Persuasively, the choice of platform should align with Nipah’s epidemiology and public health needs. Given the virus’s high fatality rate (40–75%) and sporadic outbreaks, a vaccine must be both effective and deployable under urgent conditions. mRNA’s speed and precision make it ideal for targeted interventions, whereas viral vectors’ durability and lower cost favor broader prophylactic use. Combining these platforms—a prime-boost strategy—could maximize immunity, though this requires rigorous clinical validation.
Comparatively, other platforms like protein subunit vaccines (e.g., Novavax’s COVID-19 vaccine) and DNA vaccines offer alternatives but lag in Nipah-specific development. Protein subunit vaccines, while safe and stable, may require adjuvants and multiple doses, complicating logistics. DNA vaccines, though promising in preclinical studies, face challenges in achieving sufficient immune responses without electroporation delivery systems. Ultimately, mRNA and viral vector platforms lead the race, balancing innovation, feasibility, and urgency in the fight against Nipah virus.
Part-Time Bank Teller Hours: Flexible Schedules and Work-Life Balance
You may want to see also
Explore related products






![]()
Clinical Trials: Updates on human testing phases and safety data
The development of a Nipah virus vaccine has been a critical focus in global health research, given the virus's high mortality rate and potential for outbreaks. As of recent updates, several vaccine candidates have progressed through preclinical stages, with a few now entering human testing phases. These clinical trials are pivotal in determining the safety, immunogenicity, and efficacy of potential vaccines, ensuring they meet rigorous standards before widespread use.
In the Phase I trials, the primary objective is to assess safety and dosage in healthy adults. For instance, one leading candidate, a recombinant vesicular stomatitis virus (rVSV)-based vaccine, has been administered in escalating doses ranging from 10^5 to 10^7 plaque-forming units (PFU). Early data indicates that the vaccine is well-tolerated, with mild to moderate adverse effects such as headache, fatigue, and injection site pain reported in less than 10% of participants. These trials typically involve small cohorts, often between 20 to 50 individuals, aged 18 to 55, to ensure a controlled environment for monitoring reactions.
Transitioning to Phase II, the focus shifts to evaluating immunogenicity and refining dosage regimens. Here, larger groups of participants, often including diverse age categories (e.g., adolescents and elderly individuals), are enrolled to assess how different populations respond to the vaccine. Preliminary results from ongoing trials suggest that the rVSV-based vaccine elicits a robust neutralizing antibody response in over 90% of recipients after a single dose. However, researchers are exploring whether a booster dose could enhance long-term immunity, particularly in immunocompromised individuals.
Phase III trials, though not yet initiated for Nipah virus vaccines, will be crucial for evaluating efficacy in real-world settings. These trials typically involve thousands of participants in regions endemic to Nipah virus, such as parts of South and Southeast Asia. A key challenge will be demonstrating the vaccine’s ability to prevent infection or reduce disease severity, which may require innovative trial designs given the sporadic nature of Nipah outbreaks.
Safety data across all phases remains a top priority. Continuous monitoring for rare adverse events, such as vaccine-associated enhanced disease, is essential. For example, post-vaccination follow-up periods of up to 12 months are being implemented to detect any delayed reactions. Additionally, pregnant individuals and those with pre-existing conditions are often excluded from early trials but will be included in later stages to ensure comprehensive safety profiles.
Practical tips for participants in Nipah virus vaccine trials include maintaining a symptom diary, promptly reporting any unusual reactions, and adhering to scheduled follow-up visits. For researchers, ensuring transparent communication of trial results and addressing public concerns about vaccine safety will be vital for building trust and facilitating eventual vaccine deployment. As these trials progress, their outcomes will not only shape the future of Nipah virus prevention but also contribute to broader advancements in emerging infectious disease preparedness.
Seamlessly Connect QuickBooks to Your Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Global Accessibility: Plans for distribution and affordability in affected regions
The Nipah virus, a zoonotic pathogen with a high mortality rate, primarily affects regions in South and Southeast Asia. As researchers edge closer to developing a viable vaccine, the focus shifts to ensuring its accessibility in affected areas. Distribution and affordability are critical to mitigating outbreaks, yet these challenges are compounded by logistical hurdles, economic disparities, and healthcare infrastructure limitations. Addressing these issues requires a multifaceted approach that balances innovation with practicality.
One key strategy involves leveraging existing healthcare networks in endemic regions, such as India, Bangladesh, and Malaysia. For instance, integrating Nipah vaccine distribution into routine immunization programs could streamline delivery. However, this approach necessitates training healthcare workers to handle the vaccine, which may require cold chain storage. A single-dose regimen, if proven effective, would simplify administration and reduce costs compared to multi-dose protocols. For example, a vaccine requiring storage at 2–8°C could utilize existing refrigeration systems, while a room-temperature-stable formulation would be ideal for remote areas with unreliable electricity.
Affordability remains a significant barrier, particularly in low-income communities. Public-private partnerships could subsidize vaccine costs, ensuring accessibility for vulnerable populations. A tiered pricing model, where high-income countries pay a premium to offset costs for low-income nations, has proven effective for vaccines like HPV. Additionally, global health organizations such as Gavi could play a pivotal role in financing procurement and distribution. For context, a target price of $5–10 per dose would align with affordability thresholds in affected regions, considering the economic impact of Nipah outbreaks on local economies.
Logistical challenges, such as reaching remote villages during monsoon seasons, demand innovative solutions. Drone technology, already piloted in countries like Ghana for vaccine delivery, could be adapted for Nipah-affected areas. Mobile vaccination clinics, staffed by local health workers, would ensure coverage in hard-to-reach locations. Community engagement is equally vital; awareness campaigns in local languages can dispel vaccine hesitancy and encourage uptake. For example, targeting age groups most at risk, such as adults aged 15–45 who interact with livestock or consume contaminated fruits, could maximize impact.
In conclusion, ensuring global accessibility of a Nipah virus vaccine requires a combination of strategic distribution, cost-effective pricing, and innovative delivery methods. By addressing these challenges head-on, stakeholders can transform a scientific breakthrough into a tangible public health solution, safeguarding communities from this deadly virus.
Reconciling ATM Withdrawals: How Banks Ensure Accuracy
You may want to see also
Explore related products






![]()
Effectiveness: Expected efficacy against Nipah virus strains and duration of protection
The quest for a Nipah virus vaccine has yielded several candidates, each with varying levels of expected efficacy and protection duration. Among the most promising is the recombinant vesicular stomatitis virus (rVSV)-based vaccine, which has shown significant potential in preclinical trials. This vaccine, designed to express the Nipah virus glycoprotein, has demonstrated robust immune responses in animal models, particularly in ferrets and African green monkeys. Early data suggest that a single dose could provide substantial protection against lethal Nipah virus challenge, with efficacy rates exceeding 80% in these studies. However, translating these findings to humans requires careful consideration of dosage, administration routes, and potential side effects.
From an analytical perspective, the efficacy of Nipah virus vaccines hinges on their ability to elicit neutralizing antibodies and T-cell responses. Studies indicate that a dose of 5 × 10⁶ plaque-forming units (PFU) of the rVSV-based vaccine may be sufficient to achieve protective immunity in non-human primates. This dosage strikes a balance between immunogenicity and safety, minimizing adverse reactions while ensuring robust protection. For humans, clinical trials will need to refine this dosage, potentially tailoring it to age groups—adults, adolescents, and children—to account for differences in immune response. For instance, older adults may require a higher dose or an adjuvanted formulation to overcome age-related immune decline.
Instructively, the duration of protection is a critical factor in vaccine deployment strategies. Preclinical data suggest that the rVSV-based vaccine could provide immunity for at least 12 months, with some studies indicating persistence up to 18 months. However, real-world effectiveness may vary based on factors like viral strain diversity and individual immune status. To maximize protection, a booster dose may be recommended 6–12 months after the initial vaccination, particularly in high-risk populations such as healthcare workers or those in outbreak-prone regions. Practical tips include monitoring antibody titers post-vaccination to assess the need for boosters and ensuring cold chain maintenance to preserve vaccine efficacy during distribution.
Comparatively, Nipah virus vaccines face unique challenges compared to vaccines for more common pathogens like influenza or SARS-CoV-2. Unlike these viruses, Nipah has a limited but highly lethal outbreak history, making large-scale clinical trials ethically and logistically complex. As a result, efficacy estimates rely heavily on animal models and immunological correlates of protection. This contrasts with vaccines like mRNA-based COVID-19 vaccines, which were rapidly tested in large human populations. Despite these hurdles, the Nipah vaccine’s potential for cross-protection against related henipaviruses, such as Hendra virus, adds value to its development, offering a broader public health impact.
Persuasively, investing in Nipah virus vaccine research is not just a scientific endeavor but a public health imperative. The virus’s high fatality rate (40–75%) and potential for human-to-human transmission underscore the need for a proactive approach. While current candidates show promise, their effectiveness against emerging Nipah strains remains uncertain. Ongoing research must prioritize strain surveillance and vaccine adaptability to ensure broad-spectrum protection. For policymakers, this means allocating resources for Phase III trials and establishing stockpiles for rapid deployment during outbreaks. For individuals, staying informed about vaccine availability and adhering to recommended schedules will be key to mitigating Nipah’s threat.
Verify Your Nepal Vaccine Certificate: A Step-by-Step Guide
You may want to see also
Frequently asked questions
The Nipah virus is a zoonotic virus (it is transmitted from animals to humans) that can cause severe respiratory illness and encephalitis (brain inflammation) in humans. It was first identified in 1998 in Malaysia and Singapore.
A: Currently, there is no licensed vaccine available for humans to prevent Nipah virus infection, although several candidates are in development.
A: Several vaccine candidates are being researched, including recombinant vesicular stomatitis virus (rVSV)-based vaccines, adenovirus-based vaccines, and subunit protein vaccines. Some of these candidates have shown promising results in preclinical and early clinical trials.
A: Various organizations, including the World Health Organization (WHO), Coalition for Epidemic Preparedness Innovations (CEPI), and pharmaceutical companies, are collaborating to accelerate the development of a Nipah virus vaccine.
A: The development of a vaccine is a complex and time-consuming process, involving preclinical testing, clinical trials, and regulatory approval. While progress is being made, it is challenging to predict an exact timeline for the availability of a licensed Nipah virus vaccine. However, ongoing research and funding efforts aim to expedite the process and make a vaccine available as soon as possible.































