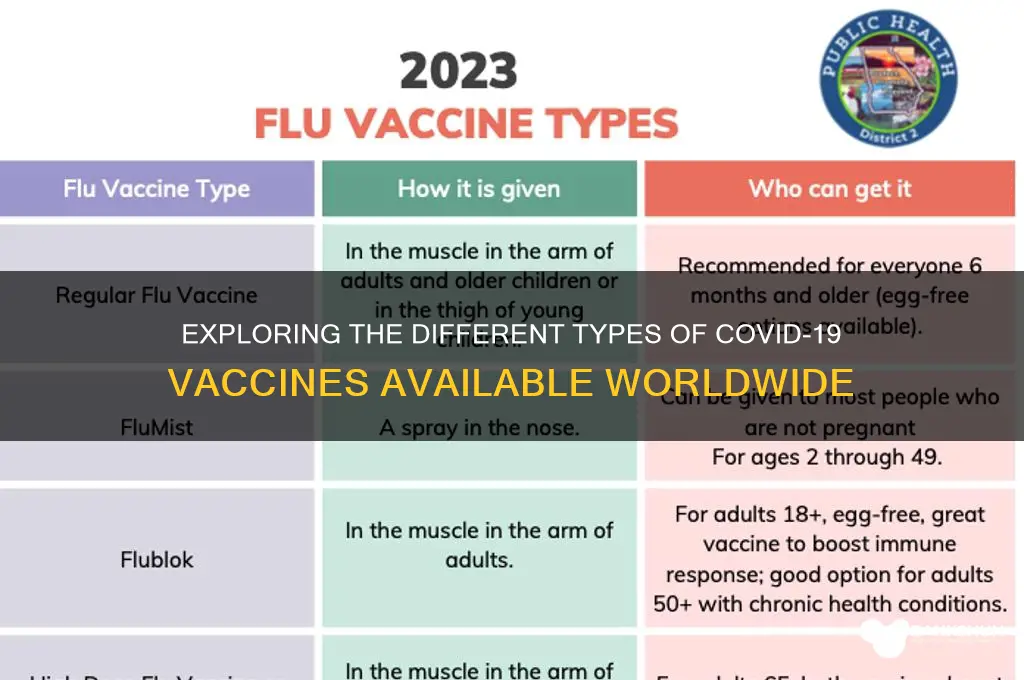
There are several types of COVID-19 vaccines developed to combat the coronavirus pandemic, each utilizing different technologies to trigger an immune response. The most widely used are mRNA vaccines, such as Pfizer-BioNTech and Moderna, which teach cells to produce a harmless protein that triggers antibody production. Viral vector vaccines, like AstraZeneca and Johnson & Johnson, use a modified virus to deliver genetic material into cells, prompting an immune response. Protein subunit vaccines, including Novavax, contain harmless pieces of the virus to stimulate immunity. Additionally, inactivated vaccines, such as Sinovac and Sinopharm, use a killed version of the virus to build protection. Each type has its unique advantages and efficacy rates, contributing to global vaccination efforts.
| Characteristics | Values |
|---|---|
| Vaccine Types | mRNA, Viral Vector, Protein Subunit, Inactivated Virus, DNA |
| Examples (mRNA) | Pfizer-BioNTech (Comirnaty), Moderna (Spikevax) |
| Examples (Viral Vector) | Oxford-AstraZeneca (Vaxzevria), Johnson & Johnson (Janssen), Sputnik V |
| Examples (Protein Subunit) | Novavax (Nuvaxovid), Abdala, ZF2001 |
| Examples (Inactivated Virus) | Sinopharm (BBIBP-CorV), Sinovac (CoronaVac), Covaxin |
| Examples (DNA) | ZyCoV-D |
| Administration Route | Intramuscular (most), Intradermal (ZyCoV-D) |
| Dose Regimen | Typically 2 doses (mRNA, Viral Vector, Protein Subunit), 1 dose (J&J) |
| Booster Recommendation | Recommended for enhanced immunity and protection against variants |
| Efficacy (Approx.) | 90-95% (mRNA), 60-90% (Viral Vector, Protein Subunit), 50-80% (Inactivated) |
| Storage Requirements | Ultra-cold (-70°C, mRNA), Refrigerated (2-8°C, most others) |
| Common Side Effects | Pain at injection site, fatigue, headache, muscle pain, fever |
| Approval Status | Emergency Use Authorization (EUA) or full approval in various countries |
| Target Population | Adults and adolescents (age varies by vaccine and country) |
| Variant Coverage | Original strain, with updated boosters for Omicron variants |
| Development Timeline | Accelerated due to global pandemic, typically 1-2 years |
| Manufacturers | Pfizer, Moderna, AstraZeneca, Johnson & Johnson, Sinopharm, Sinovac, etc. |
Explore related products






What You'll Learn
![]()
mRNA Vaccines (Pfizer, Moderna)
MRNA vaccines, pioneered by Pfizer-BioNTech and Moderna, represent a groundbreaking approach to combating COVID-19. Unlike traditional vaccines that use weakened viruses or viral proteins, these vaccines deliver genetic instructions—specifically, messenger RNA (mRNA)—to our cells. This mRNA acts as a blueprint, teaching cells to produce a harmless piece of the SARS-CoV-2 spike protein, which triggers an immune response. This innovative technology not only offers rapid development but also high efficacy, with both vaccines demonstrating around 95% effectiveness in preventing symptomatic COVID-19 in clinical trials.
The Pfizer-BioNTech vaccine, approved for individuals aged 5 and older, requires a two-dose primary series, administered 3–4 weeks apart, followed by booster shots to maintain immunity. Each dose contains 30 micrograms of mRNA for those aged 12 and up, while children 5–11 receive a lower 10-microgram dose. Moderna’s vaccine, approved for individuals aged 6 months and older, also follows a two-dose regimen but with a longer 4–8 week interval between doses. Adults receive 100 micrograms per dose, while children 6 months to 5 years receive 25–50 micrograms, depending on age. Both vaccines necessitate storage at ultra-cold temperatures initially, though Pfizer’s can now be stored in standard freezers for up to two weeks, easing distribution challenges.
One of the most compelling advantages of mRNA vaccines is their adaptability. Since they rely on synthesizing mRNA rather than culturing viruses, manufacturers can quickly modify the vaccine to target new variants, such as Omicron. This flexibility positions mRNA technology as a cornerstone for future pandemic responses. However, this innovation comes with unique considerations: mRNA vaccines are highly perishable and require precise handling, from storage to administration. Patients must also be aware of potential side effects, including fatigue, headache, and injection site pain, which are generally mild and short-lived but signal a robust immune response.
For those hesitant about mRNA vaccines, understanding their safety profile is crucial. Both Pfizer and Moderna vaccines have undergone rigorous testing and continuous monitoring, with data from billions of doses administered globally. While rare side effects like myocarditis (heart inflammation) have been reported, primarily in young males after the second dose, the risks are significantly outweighed by the vaccines’ benefits in preventing severe COVID-19. Practical tips for recipients include scheduling doses when you can rest afterward, staying hydrated, and using over-the-counter pain relievers if needed—though these should be avoided preemptively unless advised by a healthcare provider.
In conclusion, mRNA vaccines from Pfizer and Moderna exemplify the fusion of scientific ingenuity and public health necessity. Their rapid development, high efficacy, and adaptability make them a pivotal tool in the fight against COVID-19. By understanding their mechanisms, dosages, and practicalities, individuals can make informed decisions, contributing to both personal and community protection. As this technology evolves, its potential extends far beyond COVID-19, promising a new era in vaccine development.
Cracking the Piggy Bank Strategy in WSOP: A Comprehensive Guide
You may want to see also
Explore related products


$18.59 $19.95




![]()
Viral Vector Vaccines (AstraZeneca, Johnson & Johnson)
Viral vector vaccines represent a unique approach in the fight against COVID-19, leveraging modified viruses to deliver genetic instructions to our cells. AstraZeneca and Johnson & Johnson’s vaccines are prime examples of this technology, using harmless adenoviruses as vehicles to transport SARS-CoV-2 spike protein genes into the body. Once inside, these genes prompt cells to produce the spike protein, triggering an immune response without causing COVID-19. This method contrasts with mRNA vaccines, which use genetic material directly, and inactivated or protein subunit vaccines, which rely on whole or partial viral components.
Consider the administration process: AstraZeneca’s vaccine typically requires two doses, spaced 4 to 12 weeks apart, depending on local guidelines. Johnson & Johnson’s vaccine, however, stands out as a single-dose option, making it logistically simpler and appealing for populations with limited access to healthcare. Both vaccines are stored at standard refrigerator temperatures (2°C to 8°C), enhancing their distribution feasibility, especially in low-resource settings. However, their efficacy rates differ slightly, with AstraZeneca reporting around 70-80% effectiveness against symptomatic COVID-19 and Johnson & Johnson around 66-72%, though both offer strong protection against severe disease and hospitalization.
One critical aspect to note is the rare but serious side effect of thrombosis with thrombocytopenia syndrome (TTS) associated with these vaccines. This condition involves blood clots combined with low platelet counts, occurring more frequently in younger adults, particularly women under 50. Health authorities recommend monitoring for symptoms such as persistent headaches, blurred vision, or abdominal pain within 3 weeks of vaccination. While the risk is extremely low (approximately 1 in 100,000 doses), it underscores the importance of informed decision-making and prompt medical attention if symptoms arise.
From a global health perspective, viral vector vaccines have played a pivotal role in addressing vaccine inequity. Their ease of storage and single-dose option (in the case of Johnson & Johnson) have made them accessible in regions with limited infrastructure. For instance, COVAX, the global vaccine-sharing initiative, has distributed millions of AstraZeneca doses to low-income countries. This highlights their value not just as medical tools but as instruments of equity in the pandemic response.
In practice, individuals considering these vaccines should weigh their benefits against potential risks, especially if they fall into higher-risk categories for TTS. Pregnant individuals, for example, should consult healthcare providers, as data on vaccine safety in pregnancy is still evolving. For most people, however, the protection offered by viral vector vaccines far outweighs the risks, particularly in areas with high COVID-19 transmission. As with any vaccine, staying informed through trusted sources and following local health guidelines ensures the best outcomes.
Is Cash App a Third-Party Bank? Understanding Its Financial Role
You may want to see also
Explore related products




![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UY218_.jpg)

![]()
Inactivated Virus Vaccines (Sinovac, Sinopharm)
Inactivated virus vaccines, such as Sinovac (CoronaVac) and Sinopharm (BBIBP-CorV), work by using a killed version of the SARS-CoV-2 virus to trigger an immune response. Unlike live vaccines, these pose no risk of causing the disease they aim to prevent, making them a safer option for individuals with compromised immune systems. Both vaccines are administered in a two-dose regimen, typically given 3–4 weeks apart, though some countries have adopted longer intervals to potentially enhance efficacy. They are stored at standard refrigerator temperatures (2°–8°C), which simplifies distribution, especially in regions with limited cold-chain infrastructure.
Sinovac’s CoronaVac and Sinopharm’s BBIBP-CorV have been widely used in low- and middle-income countries due to their accessibility and ease of storage. Clinical trials and real-world data show varying efficacy rates, with Sinopharm reporting around 78–86% effectiveness against symptomatic disease in trials, while Sinovac’s results range from 50–90% depending on the population and study. These vaccines are particularly effective at preventing severe illness and hospitalization, which aligns with their primary goal of reducing the burden on healthcare systems. They are approved for use in adults and, in some countries, adolescents aged 12 and above, with dosages typically standardized across age groups.
One of the key advantages of inactivated virus vaccines is their established technology, which has been used for decades in vaccines against diseases like influenza and hepatitis A. This familiarity fosters public trust, especially in regions where newer mRNA or viral vector vaccines may face skepticism. However, their efficacy against emerging variants like Omicron has been a concern, prompting discussions about booster doses. Both Sinovac and Sinopharm have been studied in heterologous prime-boost strategies, where a third dose of a different vaccine type (e.g., mRNA) significantly enhances immunity, offering a practical solution to waning protection.
When considering inactivated virus vaccines, it’s important to follow local health guidelines for dosing intervals and booster recommendations. For travelers, verifying the vaccine’s acceptance in destination countries is crucial, as some nations have restrictions based on vaccine type. Side effects are generally mild, including pain at the injection site, fatigue, and low-grade fever, typically resolving within a few days. Pregnant or immunocompromised individuals should consult healthcare providers, as data on these groups is still evolving. Despite debates over efficacy, these vaccines remain a vital tool in global vaccination efforts, particularly in regions with limited access to alternatives.
Step-by-Step Guide to Registering for HSBC Internet Banking Online
You may want to see also
Explore related products






![]()
Protein Subunit Vaccines (Novavax)
Protein subunit vaccines represent a targeted approach to COVID-19 immunization, and Novavax's offering, known as NVX-CoV2373 or brand name Nuvaxovid, exemplifies this category. Unlike mRNA vaccines that instruct cells to produce a viral protein, subunit vaccines directly deliver a harmless piece of the virus—in this case, the SARS-CoV-2 spike protein—to trigger an immune response. This protein is grown in a lab using an insect virus (baculovirus) and self-assembles into nanoparticles resembling the virus’s structure, but without infectious material. The vaccine also contains an adjuvant, Matrix-M, derived from tree bark, which enhances the immune response by stimulating innate immunity.
From a practical standpoint, Novavax’s vaccine is administered in two doses, typically 3–4 weeks apart, with each dose containing 5 micrograms of the spike protein. It’s approved for individuals aged 12 and older in many countries, including the U.S. and EU, and is stored at standard refrigerator temperatures (2°C to 8°C), making it logistically simpler than some other vaccines. Clinical trials demonstrated an efficacy rate of approximately 90% against symptomatic COVID-19, with a reassuring safety profile. Common side effects include injection site pain, fatigue, and headache, typically mild to moderate and resolving within a few days.
One of the persuasive arguments for Novavax is its appeal to those hesitant about newer vaccine technologies like mRNA. By relying on a more traditional platform—protein subunits have been used in vaccines for hepatitis B and HPV—it may offer psychological comfort to certain populations. Additionally, its lack of genetic material eliminates theoretical concerns about mRNA integration into human DNA, a common misconception. However, it’s important to note that Novavax’s rollout has been slower compared to Pfizer and Moderna, partly due to manufacturing delays and regulatory approvals.
Comparatively, Novavax’s subunit approach differs from viral vector vaccines (e.g., AstraZeneca, J&J) by avoiding the use of a live virus as a delivery mechanism, reducing the risk of rare side effects like thrombosis. It also contrasts with mRNA vaccines in its reliance on a purified protein rather than genetic instructions. For individuals with allergies to polyethylene glycol (PEG), a component in mRNA vaccines, Novavax provides a viable alternative. However, its efficacy against emerging variants remains under study, as with all COVID-19 vaccines.
In conclusion, Novavax’s protein subunit vaccine is a valuable addition to the global immunization toolkit, particularly for those seeking a more conventional vaccine technology. Its straightforward storage, robust efficacy, and favorable safety profile make it a practical choice, though its availability may vary by region. As with any vaccine, consulting healthcare providers for personalized advice is essential, especially for individuals with specific medical conditions or concerns.
RFK's Vaccine Plan: Unpacking His Approach and Implications
You may want to see also
Explore related products






![]()
DNA Vaccines (Under Development)
DNA vaccines represent a cutting-edge approach in the fight against coronaviruses, leveraging genetic material to train the immune system. Unlike traditional vaccines that use weakened viruses or viral proteins, DNA vaccines introduce a small, circular piece of DNA called a plasmid into the body. This plasmid contains the genetic code for a specific viral protein, typically the SARS-CoV-2 spike protein. Once inside cells, the DNA instructs them to produce this protein, triggering an immune response without causing infection. This method is not only innovative but also highly adaptable, allowing for rapid development and modification in response to emerging variants.
One of the key advantages of DNA vaccines is their stability and ease of production. Traditional vaccines often require refrigeration and complex manufacturing processes, but DNA vaccines can be stored at room temperature and produced more efficiently. For instance, a single plasmid can be synthesized in large quantities using bacterial fermentation, reducing costs and increasing accessibility. This makes DNA vaccines particularly promising for low-resource settings where cold chain logistics are challenging. However, their efficacy remains under investigation, with clinical trials focusing on optimal dosage and delivery methods. Current studies suggest that doses ranging from 1 to 2 milligrams of DNA may be sufficient to elicit a robust immune response, though this varies based on the delivery system used.
Delivery is a critical factor in the success of DNA vaccines. Since DNA is large and negatively charged, it struggles to penetrate cell membranes on its own. Researchers have developed various methods to overcome this hurdle, including electroporation, which uses electrical pulses to create temporary pores in cell membranes, allowing DNA to enter. Another approach involves encapsulating DNA in nanoparticles or using gene guns to deliver it directly into cells. Each method has its pros and cons; for example, electroporation has shown higher efficacy but may cause more discomfort at the injection site. Practical tips for recipients include staying hydrated and applying a cold compress post-vaccination to minimize side effects.
Comparatively, DNA vaccines offer unique benefits over mRNA vaccines, another genetic-based approach. While mRNA vaccines, like Pfizer and Moderna’s, have proven highly effective, they require ultra-cold storage and degrade quickly. DNA vaccines, on the other hand, are more stable and less expensive to produce. However, they have faced challenges in generating strong enough immune responses in humans, which has slowed their progress. Ongoing research is exploring combinations of DNA vaccines with other platforms, such as protein subunit vaccines, to enhance efficacy. For instance, a prime-boost strategy—using a DNA vaccine as the first dose and a protein subunit as the second—has shown promise in preclinical studies.
Despite their potential, DNA vaccines for COVID-19 remain in the experimental stage, with no approved options available yet. Several candidates are in Phase I and II clinical trials, targeting diverse populations, including children and immunocompromised individuals. For parents considering future DNA vaccines for their children, it’s important to note that these vaccines are designed to be safe and non-infectious, as they do not contain live virus. Additionally, their ability to be quickly updated to target new variants makes them a valuable tool in long-term pandemic management. As research progresses, DNA vaccines could revolutionize not only coronavirus prevention but also the development of vaccines for other infectious diseases.
A Step-by-Step Guide to Investing in YES Bank's FPO
You may want to see also
Frequently asked questions
The main types of COVID-19 vaccines include mRNA vaccines (e.g., Pfizer-BioNTech, Moderna), viral vector vaccines (e.g., Johnson & Johnson, AstraZeneca), and protein subunit vaccines (e.g., Novavax).
mRNA vaccines teach cells to produce a harmless piece of the SARS-CoV-2 spike protein, triggering an immune response that protects against COVID-19 without using live virus.
Viral vector vaccines (e.g., Johnson & Johnson) use a modified virus to deliver genetic instructions to cells, while mRNA vaccines (e.g., Pfizer, Moderna) use messenger RNA to instruct cells to produce a viral protein, both prompting an immune response.