In 1981, the vaccination schedule was a critical component of public health efforts worldwide. This period saw the continued emphasis on immunizing children against common diseases such as measles, mumps, and rubella, as well as the introduction of new vaccines. For instance, the hepatitis B vaccine was becoming more widely available, particularly for high-risk groups. Additionally, the polio vaccination campaign was ongoing, with efforts to eradicate the disease globally. The schedule typically included multiple doses of each vaccine, administered at specific intervals to ensure optimal protection. Public health campaigns during this time focused on educating parents about the importance of adhering to the vaccination schedule to prevent the spread of infectious diseases and protect community health.
| Characteristics | Values |
|---|---|
| Year | 1981 |
| Vaccines Recommended | Measles, Mumps, Rubella (MMR), Diphtheria, Tetanus, Pertussis (DTP), Polio, Influenza |
| Age Groups | Infants (0-1 year), Toddlers (1-2 years), Preschoolers (2-5 years), School-age children (5-12 years), Adolescents (12-18 years) |
| Dosage Schedule | Varies by vaccine; typically includes multiple doses at specific intervals (e.g., MMR: 2 doses at 12 and 18 months) |
| Administration Routes | Injection (most vaccines), Oral (Polio), Nasal (Influenza) |
| Notable Changes | Introduction of the MMR vaccine, Increased emphasis on DTP vaccination |
| Public Health Campaigns | Measles eradication campaigns, Polio vaccination drives |
| Vaccine Coverage Rates | Varied by region and vaccine; generally lower than current standards |
| Side Effects | Common side effects included fever, redness, and swelling at injection site; rare serious reactions |
| Contraindications | Certain medical conditions, allergies, or previous adverse reactions |
| Global Considerations | Different countries had varying vaccination schedules and recommendations based on local disease prevalence and healthcare infrastructure |
Explore related products






What You'll Learn
- Vaccines Introduced: New vaccines added to the schedule in 1981, such as the MMR vaccine
- Recommended Ages: Specific age recommendations for each vaccine, including boosters and initial doses
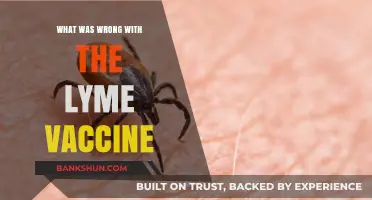
- Vaccination Coverage: Percentage of the population vaccinated against different diseases in 1981
- Public Health Campaigns: Initiatives and campaigns launched to promote vaccination and address hesitancy
- Vaccine Safety and Efficacy: Studies and data on the safety and effectiveness of vaccines available in 1981
![]()
Vaccines Introduced: New vaccines added to the schedule in 1981, such as the MMR vaccine
In 1981, the vaccination schedule saw significant updates with the introduction of new vaccines, notably the MMR vaccine. This marked a pivotal moment in public health as the MMR vaccine combined protection against three serious diseases: measles, mumps, and rubella. Prior to this, each disease had its own separate vaccine, which made immunization more complex and less accessible. The consolidation into a single shot was a major advancement, simplifying the vaccination process and improving compliance rates.
The introduction of the MMR vaccine was part of a broader effort to streamline and enhance the effectiveness of the vaccination schedule. This period also saw increased awareness and education campaigns aimed at parents and healthcare providers, emphasizing the importance of timely vaccinations. The MMR vaccine's debut was accompanied by rigorous testing and monitoring to ensure its safety and efficacy, which helped build public trust in the new immunization.
One unique aspect of the 1981 vaccination schedule was the emphasis on integrating new vaccines without disrupting the existing framework. This required careful planning and coordination to ensure that the new vaccines could be administered alongside traditional ones without causing confusion or gaps in coverage. The success of this integration paved the way for future updates to the vaccination schedule, making it more adaptable and responsive to emerging health threats.
The impact of the MMR vaccine's introduction extended beyond immediate health benefits. It also had long-term implications for public health policy and vaccine development. The success of the MMR vaccine demonstrated the potential for combination vaccines to improve immunization rates and reduce the burden of vaccine administration. This led to further research and development in the field, resulting in additional combination vaccines and more efficient vaccination strategies.
In conclusion, the introduction of the MMR vaccine in 1981 was a significant milestone in the history of vaccination schedules. It not only provided enhanced protection against three serious diseases but also set the stage for future advancements in vaccine technology and public health policy. The careful integration of this new vaccine into the existing schedule demonstrated the importance of thoughtful planning and coordination in ensuring the effectiveness and accessibility of immunization programs.
World Bank's Role in Shaping Global Politics and Governance
You may want to see also
Explore related products






![]()
Recommended Ages: Specific age recommendations for each vaccine, including boosters and initial doses
In 1981, the vaccination schedule included specific age recommendations for each vaccine, reflecting the medical understanding and public health priorities of the time. For instance, the measles vaccine was typically administered to children around 12 months of age, with a booster shot recommended between 4 to 6 years old. This schedule was designed to ensure that children were protected against measles before they entered school, where the risk of exposure was higher.
The polio vaccine, another critical component of the 1981 vaccination schedule, was given in multiple doses starting at 2 months of age, with additional doses at 4 months, 6 months, and a booster at 4 to 6 years old. This regimen was aimed at providing robust protection against polio, a disease that was still a significant public health concern at the time.
For the diphtheria, pertussis, and tetanus (DPT) vaccine, the schedule included a series of shots starting at 2 months of age, with subsequent doses at 4 months, 6 months, and a booster at 4 to 6 years old. This vaccine was crucial for protecting children against these serious bacterial diseases, which could cause severe respiratory and neurological symptoms.
The rubella vaccine, often given in combination with the measles vaccine (MMR), was recommended for children around 12 months of age, with a booster shot typically administered between 4 to 6 years old. This schedule was important for preventing rubella, which could cause serious complications, especially if contracted during pregnancy.
It's important to note that the vaccination schedule in 1981 was based on the best available medical knowledge and public health data at the time. Since then, vaccination recommendations have evolved as new vaccines have been developed and our understanding of disease transmission and prevention has improved.
Can Vaccines Be Reversed? Debunking Myths and Understanding Immunization
You may want to see also
Explore related products






![]()
Vaccination Coverage: Percentage of the population vaccinated against different diseases in 1981
In 1981, the vaccination landscape was marked by varying degrees of coverage across different diseases. One of the most significant achievements was the widespread vaccination against smallpox, which had been successfully eradicated globally just a year earlier in 1980. This monumental effort was led by the World Health Organization (WHO) and involved extensive vaccination campaigns that reached even the most remote populations.
Another disease that saw substantial vaccination efforts in 1981 was polio. The Global Polio Eradication Initiative, launched in 1988, was already underway, and vaccination coverage was increasing steadily. In many countries, polio vaccination was part of the routine immunization schedule, and mass vaccination campaigns were conducted to boost coverage.
Measles vaccination was also a priority, with many countries implementing measles vaccination programs as part of their routine immunization schedules. The measles vaccine had been available since the 1960s, and its effectiveness in preventing the disease was well-established. However, coverage varied widely between countries, with some regions achieving high vaccination rates while others lagged behind.
Other diseases that were part of the vaccination schedule in 1981 included diphtheria, pertussis (whooping cough), and tetanus. These vaccines were typically administered as part of a combined vaccine known as the DPT (diphtheria, pertussis, and tetanus) vaccine. Vaccination against these diseases was considered essential, as they were common and could cause severe illness or death.
One of the challenges in 1981 was ensuring equitable access to vaccines. While many developed countries had well-established vaccination programs, developing countries often faced barriers such as limited resources, inadequate healthcare infrastructure, and political instability. These challenges made it difficult to achieve high vaccination coverage in some regions.
In conclusion, the vaccination schedule in 1981 was focused on several key diseases, including smallpox, polio, measles, diphtheria, pertussis, and tetanus. While significant progress had been made in vaccinating populations against these diseases, there were still challenges to overcome, particularly in ensuring equitable access to vaccines globally.
Step-by-Step Guide to Registering for Wema Mobile Banking Easily
You may want to see also
Explore related products






![]()
Public Health Campaigns: Initiatives and campaigns launched to promote vaccination and address hesitancy
In 1981, public health campaigns played a crucial role in promoting vaccination and addressing hesitancy. One notable initiative was the "Vaccinate Your Child" campaign launched by the Centers for Disease Control and Prevention (CDC). This campaign aimed to increase awareness about the importance of childhood vaccinations and to encourage parents to adhere to the recommended vaccination schedule. The campaign utilized various media channels, including television, radio, and print advertisements, to reach a wide audience. Additionally, the CDC collaborated with healthcare providers and community organizations to disseminate information and address concerns about vaccine safety and efficacy.
Another significant initiative in 1981 was the establishment of the National Immunization Program (NIP) by the World Health Organization (WHO). The NIP aimed to coordinate global efforts to improve vaccination coverage and to address vaccine-preventable diseases. As part of this initiative, the WHO developed guidelines for national immunization programs, provided technical assistance to member states, and facilitated the procurement and distribution of vaccines. The NIP also played a key role in promoting the Expanded Program on Immunization (EPI), which targeted six major vaccine-preventable diseases: measles, polio, tetanus, diphtheria, pertussis, and tuberculosis.
Public health campaigns in 1981 also focused on addressing specific vaccine hesitancy concerns. For example, the CDC launched a targeted campaign to address concerns about the safety of the measles, mumps, and rubella (MMR) vaccine. This campaign included educational materials for healthcare providers and parents, as well as public service announcements featuring testimonials from parents who had successfully vaccinated their children. Similarly, the WHO developed guidelines for addressing vaccine hesitancy, which emphasized the importance of building trust with communities and providing accurate information about vaccine risks and benefits.
In addition to these initiatives, public health campaigns in 1981 also utilized innovative strategies to promote vaccination. For example, some campaigns used mobile vaccination clinics to reach underserved populations, while others partnered with schools and workplaces to offer on-site vaccination services. These efforts helped to increase vaccination coverage and to address disparities in access to healthcare services.
Overall, the public health campaigns of 1981 played a vital role in promoting vaccination and addressing hesitancy. By utilizing a variety of strategies and media channels, these campaigns helped to increase awareness about the importance of vaccination and to encourage individuals to take action to protect themselves and their communities from vaccine-preventable diseases.
How Vaccines Strengthen Immunity and Protect Against Diseases Effectively
You may want to see also
Explore related products






![]()
Vaccine Safety and Efficacy: Studies and data on the safety and effectiveness of vaccines available in 1981
In 1981, the safety and efficacy of vaccines were subjects of rigorous scientific scrutiny. Studies conducted during this period focused on understanding the adverse effects and the protective capabilities of various vaccines. One notable study published in the Journal of the American Medical Association (JAMA) examined the safety of the diphtheria, pertussis, and tetanus (DPT) vaccine, which was a critical component of the childhood vaccination schedule. The research found that while the DPT vaccine was associated with some adverse reactions, such as fever and local swelling, these side effects were generally mild and transient. Furthermore, the study emphasized the vaccine's high efficacy in preventing the three diseases, underscoring its importance in public health.
Another significant area of research in 1981 was the development and testing of the measles, mumps, and rubella (MMR) vaccine. Clinical trials demonstrated that the MMR vaccine was safe and highly effective in preventing these three serious diseases. The vaccine's safety profile was extensively studied, with researchers concluding that the risk of adverse reactions was minimal compared to the benefits of immunization. These findings were crucial in shaping the vaccination policies of the time and contributed to the widespread adoption of the MMR vaccine in subsequent years.
In addition to these specific studies, 1981 saw a broader effort to establish comprehensive vaccination schedules based on the best available scientific evidence. Health organizations, such as the Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), played key roles in developing guidelines for vaccine administration. These guidelines took into account factors such as age, disease prevalence, and vaccine efficacy to ensure that children received the necessary immunizations at the appropriate times. The emphasis on evidence-based decision-making helped to build public trust in vaccination programs and laid the foundation for future advancements in vaccine science.
Overall, the studies and data from 1981 provided strong support for the safety and efficacy of vaccines, reinforcing their critical role in preventing infectious diseases. The research conducted during this period not only addressed specific concerns about vaccine safety but also contributed to the development of comprehensive immunization strategies that have had a lasting impact on public health.
Tyra Banks' Inspiring Words to Suni: A Powerful Message
You may want to see also
Frequently asked questions
In 1981, the commonly administered vaccines included the smallpox vaccine, polio vaccine (oral and inactivated), measles vaccine, mumps vaccine, rubella vaccine, diphtheria vaccine, pertussis vaccine, and tetanus vaccine.
In 1981, the recommended polio vaccination schedule typically included three doses of the inactivated polio vaccine (IPV) for children, with the first dose given at 2 months of age, the second at 4 months, and the third at 6 months. Additionally, children often received an oral polio vaccine (OPV) as a booster dose at 18 months.
In 1981, children were typically vaccinated against measles at 12 months of age. This was the standard recommendation for the measles vaccine at that time.
Yes, in 1981, combination vaccines were available that included multiple antigens. One common combination vaccine was the MMR vaccine, which protected against measles, mumps, and rubella. Another was the DPT vaccine, which combined diphtheria, pertussis, and tetanus vaccines.
For adults in 1981, the recommended vaccination schedule varied depending on individual circumstances and health conditions. However, generally, adults were advised to receive booster doses of the tetanus vaccine every 10 years, and some adults, especially those in high-risk groups, were recommended to receive the flu vaccine annually. Additionally, adults who had not received the smallpox vaccine as children might have been advised to get vaccinated, depending on their risk of exposure.