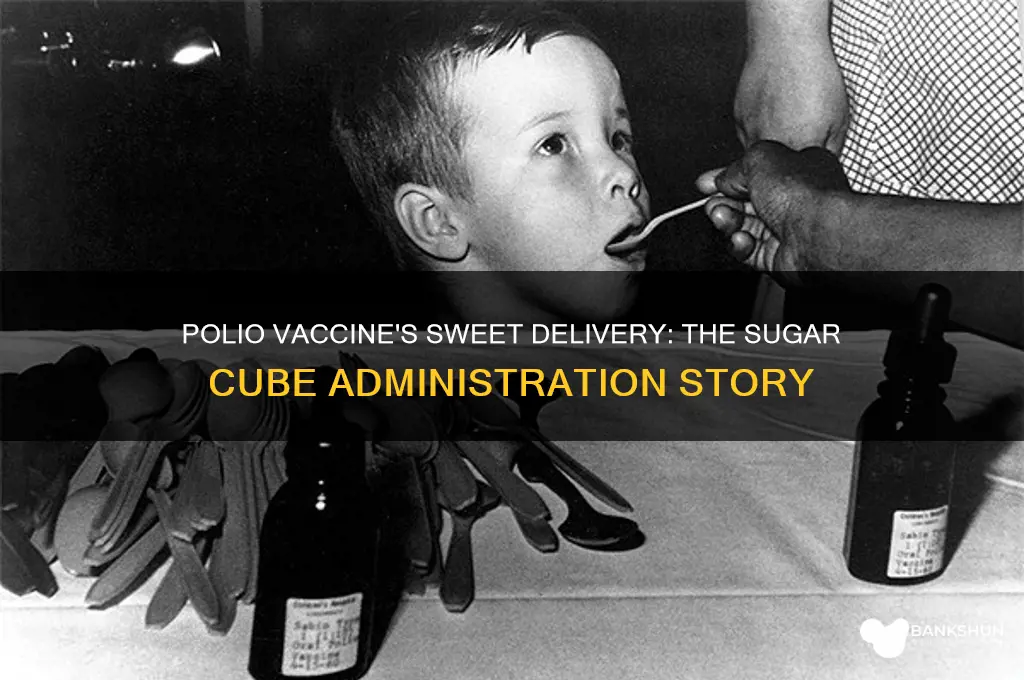
The polio vaccine administered via sugar cube became an iconic symbol of public health in the mid-20th century, particularly with the introduction of the oral polio vaccine (OPV) developed by Dr. Albert Sabin in the early 1960s. This method revolutionized polio prevention by making vaccination more accessible and appealing, especially to children. The vaccine was delivered in a liquid form that was absorbed through the lining of the mouth, and to make it more palatable, it was often placed on a small sugar cube. This approach not only ensured widespread acceptance but also facilitated mass immunization campaigns, playing a crucial role in the global effort to eradicate polio. The sugar cube method remains a memorable chapter in medical history, highlighting the creativity and innovation behind public health initiatives.
| Characteristics | Values |
|---|---|
| Vaccine Type | Oral Polio Vaccine (OPV) |
| Administration Method | Sugar cube or drops placed on a sugar cube |
| Purpose | To immunize against poliomyelitis (polio) |
| Active Ingredient | Live attenuated (weakened) poliovirus strains (Types 1, 2, and 3) |
| Dosage | Typically 1-2 drops per dose |
| Target Age Group | Infants and young children (usually starting at 6 weeks of age) |
| Number of Doses | Multiple doses (usually 3-4) administered at intervals of 4-8 weeks |
| Storage Requirement | Requires refrigeration (2°C to 8°C or 36°F to 46°F) |
| Shelf Life | Limited (typically a few months when stored properly) |
| Advantages | Easy to administer, no needles required, induces mucosal immunity |
| Disadvantages | Rare risk of vaccine-derived poliovirus (VDPV), requires cold chain |
| Historical Use | Widely used in global polio eradication campaigns (1960s-1990s) |
| Current Status | Largely replaced by inactivated polio vaccine (IPV) in many countries |
| Sugar Cube Role | Facilitated easy administration, especially in mass vaccination campaigns |
| Effectiveness | Highly effective in preventing polio transmission |
| Global Impact | Played a key role in reducing polio cases by over 99% since 1988 |
Explore related products






What You'll Learn
- Development of Sabin Vaccine: Oral polio vaccine (OPV) created by Albert Sabin, using live attenuated virus strains
- Sugar Cube Innovation: Vaccine delivered on sugar cubes to make it palatable and easy to administer
- Mass Immunization Campaigns: Global efforts in the 1960s used sugar cubes to vaccinate millions of children
- Effectiveness of OPV: Sugar cube method ensured widespread acceptance and high vaccination rates in communities
- Transition from Sugar Cubes: Later, OPV was administered via drops due to cost and logistical advantages
![]()
Development of Sabin Vaccine: Oral polio vaccine (OPV) created by Albert Sabin, using live attenuated virus strains
The Sabin vaccine, a groundbreaking oral polio vaccine (OPV), revolutionized polio eradication efforts by offering a simple, needle-free method of administration. Developed by Dr. Albert Sabin in the late 1950s, this vaccine utilized live attenuated virus strains, which were weakened to stimulate immunity without causing the disease. The innovation lay in its delivery: a few drops of the vaccine placed on a sugar cube, making it palatable and easy to administer, especially to children. This method not only increased compliance but also facilitated mass immunization campaigns, playing a pivotal role in reducing global polio cases by over 99% since its introduction.
Administering the Sabin vaccine via sugar cube was a strategic choice, combining medical efficacy with practical convenience. The sugar cube acted as both a carrier and a sweet incentive, masking the taste of the vaccine and encouraging children to take it willingly. Typically, the vaccine was administered in a dose of 0.1 mL, which was dropped onto the sugar cube and given to the recipient to consume. This method was particularly effective in large-scale campaigns, where speed and simplicity were essential. For instance, during the 1960s, millions of children in the United States and later in developing countries received the vaccine through this approach, contributing to its rapid adoption and success.
While the sugar cube method was widely embraced, it required careful handling to ensure the vaccine’s potency. The live attenuated virus strains were sensitive to heat and light, necessitating storage in a cool, dark place until administration. Health workers were trained to use sterile droppers to measure the precise dose, avoiding contamination. Parents and caregivers were also instructed to ensure the child consumed the entire sugar cube without crumbling it, as this could reduce the vaccine’s effectiveness. Despite these precautions, the simplicity of the method made it accessible even in resource-limited settings, a key factor in its global impact.
Comparing the Sabin vaccine to its predecessor, the inactivated polio vaccine (IPV) developed by Jonas Salk, highlights the advantages of the oral approach. While IPV required injection and provided primarily humoral immunity, OPV induced both systemic and mucosal immunity, preventing viral replication in the gut and reducing transmission. This dual protection made OPV a more effective tool for interrupting polio circulation in communities. However, the use of live attenuated strains in OPV carried a rare risk of vaccine-associated paralytic polio (VAPP), a concern that led to the eventual recommendation of IPV in some countries. Despite this, OPV remains the vaccine of choice for global eradication efforts due to its ease of administration and superior ability to halt viral spread.
In practice, the Sabin vaccine’s sugar cube delivery was a game-changer for public health campaigns, particularly in regions with limited healthcare infrastructure. Its success underscored the importance of designing vaccines not just for biological efficacy but also for real-world usability. For modern immunization programs, the lessons from OPV’s development and administration remain relevant: simplicity, accessibility, and cultural acceptability are as critical as scientific innovation. As we continue to combat polio and other vaccine-preventable diseases, the legacy of the Sabin vaccine serves as a reminder that the delivery method can be just as transformative as the vaccine itself.
Do Big Banks Trade the Dow? Unveiling Wall Street's Strategies
You may want to see also
Explore related products






![]()
Sugar Cube Innovation: Vaccine delivered on sugar cubes to make it palatable and easy to administer
The polio vaccine's sugar cube delivery system was a stroke of genius, transforming a potentially traumatic medical procedure into a sweet, child-friendly experience. Developed in the 1950s by Dr. Albert Sabin, the oral polio vaccine (OPV) was a live, attenuated virus suspended in a sugar solution, then absorbed onto a small, dissolvable sugar cube. This innovative method not only masked the taste of the vaccine but also simplified administration, making mass immunization campaigns feasible. For parents and healthcare workers, the sugar cube approach was a game-changer, especially when vaccinating young children who might resist injections.
Administering the polio vaccine via sugar cube was straightforward yet required precision. Each cube was infused with approximately 0.1 mL of the vaccine solution, containing around 1,000,000 plaque-forming units of the Sabin strains (Types 1, 2, and 3). The process was simple: a healthcare worker would hand the sugar cube to the child, who would then place it on their tongue, allowing it to dissolve naturally. This method was particularly effective for children aged 6 months to 5 years, the primary target group for polio vaccination. The sweetness of the cube not only encouraged compliance but also reduced anxiety, making it a preferred choice over injections in many communities.
One of the most significant advantages of the sugar cube innovation was its scalability. During the 1960s, the World Health Organization (WHO) and UNICEF launched global polio eradication campaigns, distributing millions of sugar cubes to remote and underserved areas. The cubes were lightweight, easy to transport, and did not require refrigeration, unlike some other vaccines. This logistical simplicity allowed for rapid deployment, even in regions with limited healthcare infrastructure. For instance, in India’s Pulse Polio campaign, volunteers went door-to-door, offering sugar cubes to children, contributing to the country’s polio-free status by 2014.
However, the sugar cube method was not without challenges. Ensuring the vaccine’s potency during transportation and storage was critical, as exposure to heat or moisture could render it ineffective. Additionally, the live attenuated virus in the OPV carried a rare risk of vaccine-associated paralytic polio (VAPP), prompting a shift to inactivated polio vaccine (IPV) in some regions. Despite these limitations, the sugar cube remains a symbol of medical ingenuity, demonstrating how creative delivery methods can revolutionize public health initiatives.
In practice, the sugar cube approach offers valuable lessons for modern vaccine distribution. Its success underscores the importance of designing vaccines with the end-user in mind, particularly children. For parents and caregivers, replicating the sugar cube’s appeal in today’s context could involve using flavored oral medications or edible delivery systems for other vaccines. While the sugar cube is no longer widely used for polio vaccination, its legacy endures as a testament to the power of simplicity and empathy in healthcare innovation.
Is Rand Merchant Bank Affiliated with FNB? Exploring the Connection
You may want to see also
Explore related products





![]()
Mass Immunization Campaigns: Global efforts in the 1960s used sugar cubes to vaccinate millions of children
In the 1960s, a simple sugar cube became a symbol of hope and progress in the global fight against polio. Mass immunization campaigns leveraged this unassuming vehicle to deliver the oral polio vaccine (OPV) to millions of children, transforming public health on an unprecedented scale. Developed by Dr. Albert Sabin, the OPV was a live-attenuated vaccine that could be administered orally, making it ideal for widespread distribution. The sugar cube, infused with the vaccine, was not only easy to transport and store but also palatable for children, ensuring high compliance rates. This innovative approach marked a turning point in the eradication of a disease that had once paralyzed or killed thousands annually.
The process was straightforward yet ingenious. Each sugar cube was soaked in a solution containing the OPV, providing a precise dose of 0.1 mL per cube. Health workers would carefully prepare the cubes by dipping them into the vaccine solution and allowing them to dry, ensuring the vaccine remained stable. Children, typically aged 6 months to 5 years, were given one cube to dissolve in their mouths. The sweetness of the sugar masked any medicinal taste, making the experience less intimidating for young recipients. This method was particularly effective in low-resource settings, where traditional injection-based vaccines were logistically challenging to administer.
One of the most remarkable aspects of these campaigns was their global reach. From the bustling streets of India to the remote villages of Africa, sugar cubes became a universal tool for immunization. In the United States, the "Sabin Sundays" campaigns saw millions of children receive the vaccine in schools, clinics, and community centers. Similarly, the World Health Organization (WHO) and UNICEF spearheaded efforts in developing countries, where door-to-door vaccination drives ensured even the most isolated populations were protected. By 1965, over 100 million children worldwide had been immunized using this method, drastically reducing polio cases and paving the way for future eradication efforts.
However, the success of the sugar cube campaigns was not without challenges. Maintaining the vaccine's potency during transportation and storage was critical, as the OPV required refrigeration until use. Health workers had to be trained to handle the vaccine properly, and public education campaigns were essential to dispel myths and build trust. Despite these hurdles, the sugar cube method demonstrated the power of simplicity and innovation in public health. It also highlighted the importance of international collaboration, as governments, NGOs, and local communities worked together to achieve a common goal.
The legacy of these mass immunization campaigns extends far beyond the 1960s. The sugar cube method not only helped control polio but also set a precedent for future vaccination drives, including those for measles, rubella, and COVID-19. It remains a testament to human ingenuity and the impact of thinking outside the box in addressing global health challenges. Today, as we continue to combat infectious diseases, the lessons learned from this era remind us that even the smallest tools—like a sugar cube—can make a monumental difference.
Second Chance Banking: Rebuilding Financial Trust and Opportunities
You may want to see also
Explore related products






![]()
Effectiveness of OPV: Sugar cube method ensured widespread acceptance and high vaccination rates in communities
The oral polio vaccine (OPV), delivered via the iconic sugar cube, revolutionized polio eradication efforts in the mid-20th century. This method wasn't just a clever gimmick; it was a strategic choice that addressed key barriers to vaccination, particularly in developing countries. Unlike injections, which require trained medical personnel and sterile equipment, the sugar cube method was simple and accessible. Community health workers or even volunteers could easily administer the vaccine, expanding reach into remote areas.
The sugar cube itself played a crucial role. Its sweetness masked the vaccine's taste, making it palatable for children, a critical demographic for polio eradication. This was especially important considering the target age group for OPV: infants and young children, typically receiving their first dose around 2 months old, followed by subsequent doses at 4 months and 6-18 months. The ease of administration and child-friendly delivery system contributed to high vaccination rates, a cornerstone of successful polio eradication campaigns.
Imagine a bustling village square. A health worker sets up a makeshift station, armed with vials of OPV and a tray of sugar cubes. Children, lured by the promise of a sweet treat, line up eagerly. This scenario, repeated countless times across the globe, illustrates the power of the sugar cube method. It transformed vaccination from a potentially intimidating medical procedure into a positive, even enjoyable, experience. This shift in perception was instrumental in overcoming vaccine hesitancy, a significant challenge in many communities.
The effectiveness of the sugar cube method extended beyond its simplicity. The OPV itself, a live attenuated vaccine, offered several advantages. It induced both humoral and mucosal immunity, providing robust protection against poliovirus. The recommended dosage, typically 2 drops per child, was easy to administer and ensured consistent delivery. Furthermore, the vaccine's stability at room temperature for a limited period allowed for wider distribution, even in areas with limited refrigeration infrastructure.
While the sugar cube method played a pivotal role in polio eradication, it's important to acknowledge its limitations. The live attenuated virus in OPV, though rare, could revert to a virulent form, causing vaccine-associated paralytic polio (VAPP). This risk, though extremely low, led to the development and eventual preference for the inactivated polio vaccine (IPV) in some countries. However, in the context of mass vaccination campaigns aimed at rapid polio eradication, the benefits of OPV's ease of administration and effectiveness outweighed the minimal risks. The sugar cube method, a testament to innovative public health strategies, remains a powerful example of how simplicity and accessibility can drive global health successes.
Understanding the Role of a Bank Compliance Manager: Duties and Responsibilities
You may want to see also
Explore related products


$16.99




![]()
Transition from Sugar Cubes: Later, OPV was administered via drops due to cost and logistical advantages
The sugar cube method of administering the oral polio vaccine (OPV) was a groundbreaking innovation in the 1950s and 1960s, but it wasn't without its challenges. While the cubes were effective in delivering the vaccine, they required a complex supply chain to maintain their integrity. The cubes had to be stored at a specific temperature, and their shelf life was limited, making distribution in remote or resource-poor areas difficult. As global vaccination campaigns expanded, the need for a more cost-effective and logistically simpler solution became apparent.
The Shift to Drops: A Practical Alternative
The transition to administering OPV via drops was driven by the need for a more efficient and accessible method. This new approach eliminated the need for specialized storage and transportation conditions, as the vaccine could be stored in vials at a wider range of temperatures. A typical dose of OPV is 0.05-0.1 mL, which can be easily administered using a dropper or a small cup. This method is particularly suitable for mass vaccination campaigns, where speed and simplicity are crucial. For instance, in a campaign targeting children under 5 years old, health workers can quickly dispense the vaccine to large numbers of children without the need for individual sugar cubes.
Cost-Effectiveness and Scalability
One of the primary advantages of the drop method is its cost-effectiveness. Producing and distributing sugar cubes required significant resources, whereas vials of OPV are cheaper to manufacture and transport. This reduction in cost enabled vaccination programs to reach more people, especially in low-income countries. Moreover, the drop method allows for easier dose adjustment, as the vaccine can be administered in smaller or larger quantities depending on the age and weight of the recipient. For example, infants may receive a smaller dose (0.05 mL) compared to older children (0.1 mL).
Practical Implementation and Tips
When administering OPV via drops, it's essential to ensure proper training for health workers. The vaccine should be stored between 2-8°C (36-46°F) and protected from light. Before administration, the vial should be shaken gently to ensure the vaccine is well-mixed. Health workers should use a clean dropper or cup for each child to prevent contamination. In areas with limited access to clean water, the vaccine can be administered directly into the mouth using a dropper. It's also crucial to monitor the cold chain to maintain the vaccine's potency, especially in hot climates.
Comparative Analysis and Takeaway
While the sugar cube method played a vital role in early polio eradication efforts, the transition to drops has been instrumental in sustaining and expanding global vaccination campaigns. The drop method's simplicity, cost-effectiveness, and scalability have made it a preferred choice for health organizations worldwide. By eliminating the logistical challenges associated with sugar cubes, the drop method has enabled more efficient vaccine distribution, ultimately contributing to the significant decline in polio cases globally. As we continue to combat polio and other vaccine-preventable diseases, the lessons learned from this transition highlight the importance of adapting vaccination strategies to meet the unique needs of diverse populations.
Understanding Your Rights as a Bank Creditor
You may want to see also
Frequently asked questions
The sugar cube was used as a delivery method for the oral polio vaccine (OPV) developed by Albert Sabin. The vaccine was placed on the sugar cube to make it easier and more palatable to administer, especially to children.
The sugar cube was soaked in a solution containing the live, attenuated polio virus. When ingested, the vaccine stimulated the immune system to produce antibodies against the virus, providing protection against polio.
No, the sugar cube method is no longer commonly used. Modern polio vaccination typically involves oral drops or injections, depending on the type of vaccine (OPV or inactivated polio vaccine, IPV). The sugar cube method was phased out due to advancements in vaccine delivery systems.