In the 1860s, the transportation of vaccines was a challenging endeavor, constrained by the limitations of the era's technology and infrastructure. Vaccines, primarily smallpox vaccines at the time, were often transported in a dried lymph form, known as scabs or threads, which were more stable than liquid vaccines but still required careful handling to maintain efficacy. These materials were typically carried in glass vials or metal containers, packed in insulating materials like cotton or wool to protect them from temperature fluctuations. Transportation relied heavily on horse-drawn carriages, trains, and ships, with journeys often taking days or weeks, during which the vaccines had to be shielded from heat, light, and contamination. Ice was occasionally used for cooling, but its availability was limited, and the lack of refrigeration posed a significant risk to vaccine viability. Despite these challenges, the efforts to distribute vaccines during this period marked a crucial step in the global fight against infectious diseases, laying the groundwork for future advancements in vaccine logistics and preservation.
| Characteristics | Values |
|---|---|
| Transport Method | Primarily by horse-drawn carriages, trains, and ships. |
| Container Type | Glass vials or ampoules, often sealed with wax or cork. |
| Cooling Mechanism | Ice packs, ice boxes, or cold water baths. No mechanical refrigeration. |
| Storage Temperature | Not strictly controlled, relied on ambient temperatures and ice. |
| Shelf Life | Limited, often only days or weeks due to lack of preservatives and temperature control. |
| Distribution Network | Localized, relying on physicians, apothecaries, and government health officials. |
| Speed of Transport | Slow, dependent on animal or steam-powered transportation. |
| Preservatives | Minimal or none, leading to rapid degradation. |
| Documentation | Handwritten records, if any, with limited tracking. |
| Regulatory Oversight | Virtually nonexistent; quality and efficacy varied widely. |
Explore related products

$17.35 $24.99





What You'll Learn
- Use of ice boxes for vaccine preservation during long-distance transportation in the 1860s
- Role of horse-drawn carriages in distributing vaccines across rural areas
- Challenges of maintaining vaccine potency without modern refrigeration methods
- Transportation networks: railways and ships in global vaccine distribution
- Local volunteers and medical teams in hand-delivering vaccines to communities
![]()
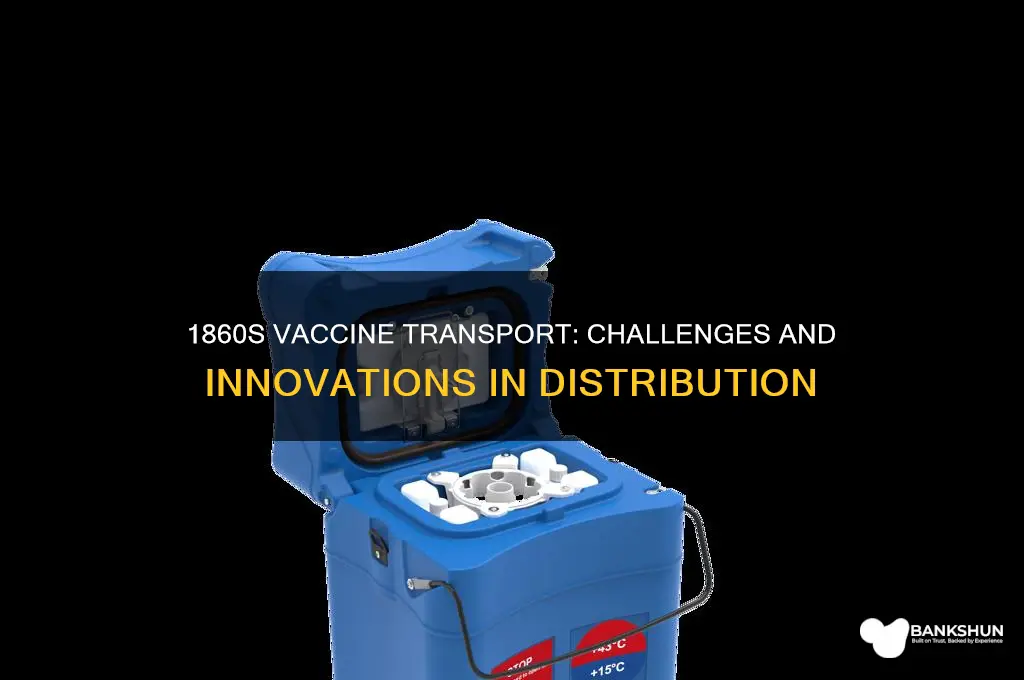
Use of ice boxes for vaccine preservation during long-distance transportation in the 1860s
In the 1860s, the transportation of vaccines over long distances presented a formidable challenge, as these biological agents required precise temperature control to remain viable. Ice boxes, rudimentary yet effective, emerged as a critical solution. Constructed from wood and lined with tin or zinc, these containers were insulated with materials like straw, sawdust, or cork to minimize heat transfer. Blocks of ice, often harvested from frozen lakes and rivers during winter, were placed around the vaccine vials to maintain a cool environment. This method, though primitive by today's standards, was a significant advancement in preserving vaccines like the smallpox vaccine, which was among the few available at the time.
The use of ice boxes required careful planning and execution. Vaccines, typically stored in glass vials, were wrapped in cotton or wool to prevent breakage and placed in the center of the ice box, farthest from the melting ice. The box was then sealed tightly to retain the cold air. For long journeys, additional ice was often packed in separate compartments or carried in reserve to replenish the melting supply. This system was particularly crucial for transporting vaccines to remote areas, where access to medical supplies was limited. However, the effectiveness of ice boxes depended heavily on external conditions, such as ambient temperature and the duration of travel, making it a delicate and unpredictable process.
One of the most notable examples of ice box usage was during the Civil War era, when smallpox outbreaks were rampant in military camps. Vaccines were transported from urban centers to field hospitals using ice boxes, often carried by horse-drawn wagons or trains. The success of these efforts was documented in medical reports, which highlighted the importance of maintaining a consistent temperature below 50°F (10°C) to ensure vaccine potency. For instance, a single dose of the smallpox vaccine, typically administered via arm-to-arm inoculation, required careful handling to remain effective for up to two weeks during transit. This period was critical, as delays could render the vaccine useless and leave populations vulnerable to disease.
Despite their utility, ice boxes had limitations that necessitated meticulous attention to detail. The ice had to be replaced regularly, which was challenging in regions without access to ice houses or natural ice sources. Additionally, the risk of contamination from melting water or improper handling posed a constant threat. Travelers and medical personnel were instructed to monitor the ice box’s internal temperature using thermometers, though these were not always reliable. Practical tips included placing the ice box in shaded areas during stops and avoiding opening it unnecessarily to preserve the cold air. These precautions, while cumbersome, were essential to ensure the vaccines reached their destination in a usable state.
In retrospect, the use of ice boxes in the 1860s marked a pivotal step in the history of vaccine logistics. It demonstrated humanity’s ingenuity in overcoming the limitations of the time and laid the groundwork for modern cold chain systems. While the technology was rudimentary, its principles—insulation, temperature control, and careful handling—remain fundamental to vaccine transportation today. The ice box era reminds us of the challenges faced by early medical pioneers and the resourcefulness required to protect public health in an age before refrigeration and rapid transportation.
Step-by-Step Guide to Setting Up Banking 365 for Beginners
You may want to see also
Explore related products



![There Was an Old Lady Who Swallowed a Truck (There Was an Old Lady [Colandro])](https://m.media-amazon.com/images/I/A1oGS0v949L._AC_UL320_.jpg)


![]()
Role of horse-drawn carriages in distributing vaccines across rural areas
In the 1860s, the distribution of vaccines across rural areas was a logistical challenge that required ingenuity and reliance on existing transportation methods. Horse-drawn carriages emerged as a vital solution, bridging the gap between urban medical centers and remote communities. These carriages, often repurposed from everyday use, were adapted to carry delicate vaccine vials, which needed protection from heat, breakage, and contamination. The role of these carriages was not merely functional but transformative, ensuring that life-saving vaccines reached those farthest from medical hubs.
Consider the practicalities: Vaccines like the smallpox vaccine, which was widely distributed during this era, required careful handling. Glass vials containing lymph from vaccinated individuals or glycerinated vaccine preparations were wrapped in cotton or wool and placed in insulated containers. These containers were then secured in padded wooden crates, often lined with straw or sawdust to absorb shocks during travel. Horse-drawn carriages, with their slower but steady pace, minimized the risk of damage compared to faster, more jarring modes of transport. Drivers were instructed to avoid rough terrain and maintain a consistent speed, typically around 5–8 miles per hour, to preserve the vaccine’s efficacy.
The use of horse-drawn carriages also addressed the issue of accessibility in rural areas, where roads were often unpaved and infrastructure limited. Unlike trains or steamships, which required specific routes and stations, carriages could navigate narrow paths and reach isolated farms or villages. This flexibility was crucial for vaccinating vulnerable populations, such as children under 5 years old, who were at higher risk of smallpox. For instance, a single carriage could carry enough vaccine doses to immunize an entire village, with each vial containing approximately 10–20 doses, depending on the method of administration.
However, this method was not without challenges. Horses required frequent rest stops, and journeys could take days or even weeks, depending on the distance. Vaccines had to be replenished or replaced if the journey exceeded their shelf life, typically 2–4 weeks under optimal conditions. Additionally, drivers and medical personnel often had to educate rural communities about the importance of vaccination, as skepticism and misinformation were common. Despite these hurdles, horse-drawn carriages remained a cornerstone of vaccine distribution, demonstrating how simple technology could be adapted to meet critical public health needs.
In conclusion, the role of horse-drawn carriages in distributing vaccines across rural areas in the 1860s was indispensable. They combined practicality, adaptability, and resilience to overcome the era’s logistical constraints. By ensuring vaccines reached remote populations, these carriages played a pivotal role in controlling diseases like smallpox, laying the groundwork for modern vaccination campaigns. Their legacy reminds us that innovation in public health often relies on leveraging available resources in creative ways.
Finding Your Bank Username: A Quick and Easy Guide
You may want to see also
Explore related products






![]()
Challenges of maintaining vaccine potency without modern refrigeration methods
In the 1860s, vaccines were primarily transported using insulated containers packed with ice, a method that seems rudimentary by today’s standards. Smallpox vaccine lymph, for instance, was often stored in glass vials nestled in ice-filled metal boxes, which were then wrapped in flannel or wool to slow heat penetration. This approach, while innovative for the time, was fraught with challenges, particularly in maintaining the potency of vaccines, which required precise temperature control to remain effective. Without modern refrigeration, the delicate balance between keeping the vaccine cool enough to prevent degradation and warm enough to avoid freezing became a logistical nightmare.
One of the primary challenges was the limited lifespan of ice during transport. Journeys often spanned days or weeks, especially in rural or colonial regions, where access to fresh ice was scarce. As ice melted, temperatures fluctuated, exposing vaccines to heat stress that could denature the active components. For example, the smallpox vaccine, which needed to be kept between 2°C and 8°C (36°F to 46°F), would lose potency rapidly if temperatures rose above this range. Travelers and medical personnel had to rely on frequent resupply of ice, a task that was both costly and logistically demanding, particularly in remote areas.
Another critical issue was the lack of reliable temperature monitoring tools. Thermometers of the era were bulky and imprecise, making it difficult to gauge whether the vaccine had been exposed to damaging temperatures. This uncertainty forced medical practitioners to discard vaccines after long journeys, even if they appeared viable, to avoid administering ineffective or harmful doses. For instance, a single vial of smallpox vaccine, containing enough lymph for 50 inoculations, could be rendered useless after just a few days of improper storage, wasting precious resources and delaying immunization efforts.
The fragility of vaccine containers further compounded these challenges. Glass vials, though effective for storage, were prone to breakage during transport, especially over rough terrain. Alternative materials like animal bladders or quills, sometimes used for smallpox vaccine lymph, were more durable but introduced risks of contamination. Without sterile packaging or preservatives, vaccines were susceptible to bacterial growth, which could render them not only ineffective but also dangerous. This duality of vulnerability—to both physical damage and biological contamination—made every step of transport a high-stakes endeavor.
Despite these obstacles, the ingenuity of 19th-century medical practitioners cannot be understated. They developed makeshift cooling systems, such as burying vaccine containers in cool earth or using evaporative cooling techniques, to extend potency. Instructions for vaccine transport often included detailed protocols, such as shielding containers from direct sunlight and avoiding jostling during travel. While these methods were far from foolproof, they highlight the resourcefulness required to combat the inherent limitations of the time. The challenges of maintaining vaccine potency without modern refrigeration underscore the remarkable progress made in vaccine logistics and storage over the past century and a half.
Understanding the Role of a Westpac Personal Banker: Duties and Benefits
You may want to see also
Explore related products




![]()
Transportation networks: railways and ships in global vaccine distribution
In the 1860s, the transportation of vaccines was a logistical challenge that relied heavily on the emerging global transportation networks of railways and ships. These networks were not only vital for the movement of goods and people but also played a critical role in the distribution of life-saving vaccines, particularly smallpox vaccine, which was the most widely used at the time. The lymph from vaccinated individuals, known as vaccine lymph, was transported in glass tubes or threads, often soaked in glycerin to preserve its potency. This delicate cargo required careful handling and timely delivery to maintain its efficacy.
Railways emerged as a key player in vaccine distribution within continents. For instance, in the United States, the expanding railroad system allowed for the rapid transport of vaccine lymph from urban centers to rural areas. The lymph was often carried in insulated containers to protect it from temperature fluctuations, which could render it ineffective. Instructions for local physicians included keeping the lymph cool and using it within a specific timeframe, typically within 5–7 days of receipt. This method significantly reduced the time it took to distribute vaccines compared to earlier, slower methods like horse-drawn carriages.
Ships, on the other hand, were indispensable for global vaccine distribution. The smallpox vaccine was transported across oceans to colonies and far-flung territories, where outbreaks were common. For example, vaccine lymph was shipped from Europe to India, a journey that could take several weeks. To ensure viability, the lymph was often transported in multiple batches, with each batch containing enough material for several vaccinations. Practical tips for sea transport included storing the lymph in dark, cool parts of the ship and avoiding exposure to extreme temperatures. Despite these precautions, the success rate of vaccine transport by sea was variable, with potency loss being a frequent issue.
A comparative analysis of railway and ship transport reveals their complementary roles. Railways offered speed and reliability over land, making them ideal for regional distribution. Ships, while slower, provided the only means of crossing continents and oceans, enabling global reach. However, the longer transit times and unpredictable conditions at sea posed greater risks to vaccine potency. This duality highlights the importance of tailoring transportation methods to the specific needs of vaccine distribution, balancing speed, cost, and preservation.
To maximize the effectiveness of these transportation networks, coordination between medical authorities, railway companies, and shipping lines was essential. For instance, in the British Empire, a system was established where vaccine lymph was regularly sent from London to colonies via scheduled ships. Local health officials were instructed to collect the lymph upon arrival and distribute it to vaccination stations. This structured approach ensured a steady supply of viable vaccine, even in remote areas. By leveraging the strengths of railways and ships, the 1860s marked a significant step forward in global vaccine distribution, laying the groundwork for modern immunization campaigns.
Effective Political Phone Banking Setup: Strategies for Successful Campaign Outreach
You may want to see also
Explore related products





![]()
Local volunteers and medical teams in hand-delivering vaccines to communities
In the 1860s, the transportation of vaccines was a labor-intensive endeavor, often reliant on human dedication rather than advanced logistics. Local volunteers and medical teams played a pivotal role in hand-delivering vaccines to communities, bridging the gap between urban medical centers and remote areas. These individuals, armed with insulated containers and a sense of urgency, traversed challenging terrains to ensure that life-saving doses reached those in need. Their efforts were not merely logistical but deeply humanitarian, as they often provided on-the-spot education about vaccination benefits and administered doses to vulnerable populations, including children and the elderly.
Consider the smallpox vaccine, one of the few available during this era. A typical dose required careful handling, as it was often transported in glass vials containing lymph material from vaccinated individuals. Local volunteers were trained to keep these vials cool using ice packs or damp cloths, though refrigeration was a luxury few could afford. For instance, a volunteer might carry enough vaccine for 50–100 doses, each requiring immediate administration upon arrival. This meant meticulous planning: mapping routes, coordinating with village leaders, and ensuring recipients were present. The success of such missions often hinged on the volunteers’ ability to navigate not just physical obstacles but also public skepticism about vaccines.
The role of medical teams was equally critical, especially in administering vaccines safely. These teams, often consisting of a physician and one or two assistants, would accompany volunteers or meet them at designated locations. Armed with lancets for scarification (the method of vaccine delivery at the time), they worked swiftly to inoculate as many people as possible. For example, a team might aim to vaccinate 30–40 individuals per day, a daunting task given the manual nature of the process. Practical tips included sterilizing tools with boiling water or alcohol and ensuring recipients avoided strenuous activity for 48 hours post-vaccination. These teams also documented outcomes, tracking success rates and adverse reactions to improve future efforts.
Comparatively, the reliance on local volunteers and medical teams highlights the stark contrast between 19th-century vaccine distribution and modern systems. Today, vaccines are transported via refrigerated trucks and global supply chains, yet the human element remains crucial in last-mile delivery. In the 1860s, however, this human element was the entire system. Volunteers and medical teams not only delivered vaccines but also built trust within communities, addressing fears and misconceptions. Their work laid the foundation for public health initiatives that continue to shape vaccination campaigns worldwide.
To replicate such efforts today in resource-limited settings, consider these steps: organize local training sessions for volunteers on vaccine handling and administration, establish clear communication channels with community leaders, and provide simple, culturally relevant educational materials. Cautions include ensuring volunteers are adequately supported to avoid burnout and verifying the cold chain (even if rudimentary) to maintain vaccine efficacy. The takeaway is clear: in the absence of advanced infrastructure, the dedication of local volunteers and medical teams remains indispensable for delivering vaccines to those who need them most.
Reset Your Yes Bank ATM PIN: A Quick and Secure Guide
You may want to see also
Frequently asked questions
Vaccines in the 1860s, primarily smallpox vaccines, were transported using lymph from vaccinated individuals or animals, often stored in glass capillary tubes or threads soaked in lymph, which were then carried in protective cases.
Preservation methods included storing lymph-soaked threads or capillary tubes in cool, dry conditions, sometimes using ice or snow for short-term transport, though long-term preservation was challenging without refrigeration.
The absence of refrigeration meant vaccines had a limited shelf life, often only days or weeks. Transport over long distances was risky, and vaccines frequently lost potency, necessitating frequent re-vaccination from fresh sources.
One innovative technique was the "arm-to-arm" method, where vaccinated individuals traveled with the vaccine in their bodies, transferring lymph to others upon arrival. This ensured a fresh supply but was labor-intensive and impractical for large-scale distribution.