The question of whether a 3rd vaccine dose and a booster shot are the same has sparked considerable discussion, particularly as vaccination strategies evolve to combat emerging variants and waning immunity. While both involve an additional dose of a vaccine, their purpose and timing can differ. A 3rd dose is often administered to individuals with weakened immune systems to ensure they achieve adequate protection, whereas a booster is typically given to the general population months after their initial series to enhance immunity that may have diminished over time. Understanding these distinctions is crucial for clarity in public health messaging and ensuring individuals receive the appropriate dose at the right time.
| Characteristics | Values |
|---|---|
| Definition | The 3rd vaccine dose and booster are not always the same. A 3rd dose is typically for immunocompromised individuals to complete their primary series, while a booster is for the general population to enhance waning immunity. |
| Purpose | 3rd Dose: Completes primary vaccination for those with weakened immune systems. Booster: Enhances immunity in the general population after the primary series. |
| Eligibility | 3rd Dose: Immunocompromised individuals (e.g., organ transplant recipients, cancer patients). Booster: General population, usually 6+ months after the primary series or last dose. |
| Timing | 3rd Dose: Administered 28 days after the 2nd dose for immunocompromised individuals. Booster: Given 6+ months after the primary series or last dose. |
| Vaccine Type | Both may use the same vaccine type (e.g., mRNA vaccines like Pfizer or Moderna), but formulations may differ (e.g., updated bivalent boosters). |
| Immune Response | 3rd Dose: Aims to achieve adequate initial immunity in immunocompromised individuals. Booster: Strengthens existing immunity in the general population. |
| FDA/CDC Guidelines | 3rd Dose: Specifically recommended for immunocompromised individuals. Booster: Recommended for the general population based on age, time since last dose, and vaccine availability. |
| Examples | 3rd Dose: Part of the primary series for immunocompromised individuals. Booster: Additional dose for the general population (e.g., bivalent COVID-19 booster). |
| Global Variations | Definitions and recommendations may vary by country based on local health authority guidelines. |
Explore related products






What You'll Learn
- Definition Differences: Third dose vs. booster: purpose, timing, and eligibility criteria explained
- Immune Response: How boosters enhance immunity compared to standard vaccine doses
- Vaccine Types: Specific vaccines requiring third doses or boosters (e.g., mRNA, viral vector)
- Global Guidelines: Varying recommendations by health organizations (WHO, CDC, EMA)
- Side Effects: Common reactions and differences between third doses and boosters
![]()
Definition Differences: Third dose vs. booster: purpose, timing, and eligibility criteria explained
The terms "third dose" and "booster" are often used interchangeably, but they serve distinct purposes in vaccination protocols. A third dose is typically administered to individuals with moderately to severely compromised immune systems, who may not have mounted a sufficient immune response after the initial vaccine series. For example, recipients of organ transplants or those undergoing cancer treatment might require this additional dose to achieve adequate protection. In contrast, a booster shot is given to individuals with healthy immune systems to enhance immunity that has waned over time. Understanding this difference is crucial for both healthcare providers and the public to ensure appropriate vaccine administration.
Timing plays a pivotal role in distinguishing between a third dose and a booster. A third dose is usually administered 28 to 30 days after the second dose in a primary vaccine series, as seen in the Pfizer-BioNTech and Moderna COVID-19 vaccines. This expedited timeline aims to bridge the immunity gap in immunocompromised individuals. Boosters, however, are given months after the completion of the primary series—for instance, the CDC recommends a COVID-19 booster 5 months after the Pfizer-BioNTech or Moderna series, or 2 months after the Johnson & Johnson vaccine. This delay allows the immune system to mature its response before reinforcement.
Eligibility criteria further highlight the differences between these doses. Third doses are specifically targeted at immunocompromised individuals, such as those on active chemotherapy or with advanced HIV. For COVID-19 vaccines, this includes people aged 5 and older with eligible conditions. Boosters, on the other hand, are recommended for a broader population, including healthy adults and adolescents. For example, Pfizer-BioNTech boosters are authorized for individuals aged 12 and older, while Moderna boosters are for those 18 and older. These criteria ensure that the right individuals receive the right dose at the right time.
Practical tips can help clarify these distinctions. If you’re immunocompromised, consult your healthcare provider to determine if a third dose is necessary, as this decision often requires medical evaluation. For boosters, stay informed about updated guidelines, as eligibility and timing may evolve with new data. Keep track of your vaccination dates to ensure compliance with recommended intervals. Finally, always verify the specific vaccine brand and dosage, as these can vary—for instance, a Pfizer booster for adolescents is a lower dose than the primary series. Understanding these nuances empowers individuals to make informed decisions about their vaccination journey.
Harvest Hope Food Bank: Fighting Hunger and Supporting Communities in Need
You may want to see also
Explore related products






![]()
Immune Response: How boosters enhance immunity compared to standard vaccine doses
Boosters are not merely repeat doses of a vaccine; they are strategically designed to amplify and refine the immune response. Unlike a third dose, which may simply aim to reinforce the initial immunity, boosters often contain a modified formulation or a higher concentration of antigen. For instance, the COVID-19 mRNA boosters (e.g., Pfizer-BioNTech or Moderna) are administered at the same dosage as the primary series but are tailored to target specific variants like Omicron. This precision ensures that the immune system not only recalls its initial response but also adapts to evolving threats, producing antibodies and memory cells with enhanced specificity and durability.
Consider the immune system as a library where vaccines are the books that teach it to recognize pathogens. The primary vaccine series builds the initial collection, but boosters act like updated editions, refining the knowledge and adding new details. For example, after a COVID-19 booster, B cells—the immune system’s antibody factories—undergo a process called affinity maturation, where they produce higher-quality antibodies that bind more effectively to the virus. This is why booster recipients often exhibit a 10- to 20-fold increase in neutralizing antibodies compared to pre-booster levels, significantly reducing the risk of severe illness.
Practical implementation of boosters varies by age and health status. For adults over 65 or immunocompromised individuals, a booster is typically recommended 6 months after the second dose of an mRNA vaccine, as their immune responses may wane faster. In contrast, younger, healthy individuals may maintain sufficient immunity for up to 8 months. A key takeaway is timing: administering a booster too early may limit the immune system’s ability to mount a robust response, while delaying it risks leaving a gap in protection. Always consult healthcare guidelines for age-specific recommendations.
To maximize the benefits of a booster, combine it with lifestyle measures that support immune health. Adequate sleep (7–9 hours per night), a diet rich in vitamins C and D, and regular physical activity can enhance the body’s response to vaccination. Avoid stressors like excessive alcohol or smoking, which can impair immune function. For those hesitant about boosters, understanding their role in preventing not just infection but also long-term complications like long COVID or multisystem inflammatory syndrome can provide a compelling rationale for staying up to date with immunizations.
In summary, boosters are a critical tool for sustaining and improving immunity, offering a targeted upgrade to the immune system’s defenses. By optimizing timing, dosage, and formulation, they ensure that the body remains prepared to combat pathogens efficiently. Whether it’s a third dose or a booster, the distinction lies in its purpose—one may complete the initial series, while the other sharpens the immune response for long-term resilience. Always follow healthcare provider guidance to determine which option aligns with your specific needs.
Enroll in Zelle with Huntington Bank: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
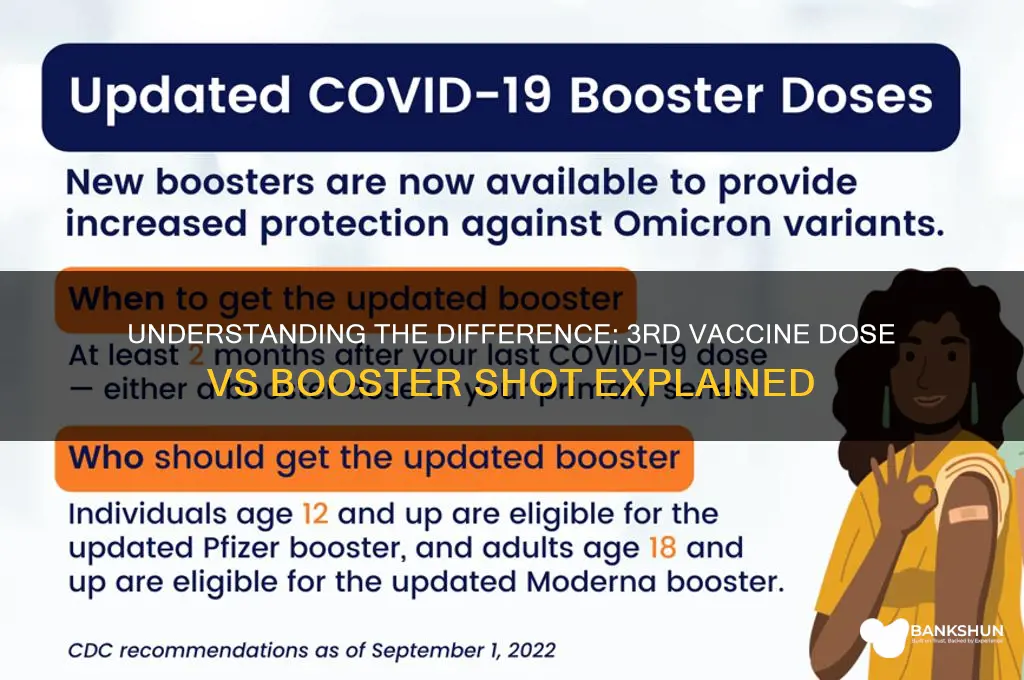
Vaccine Types: Specific vaccines requiring third doses or boosters (e.g., mRNA, viral vector)
The distinction between a third dose and a booster shot lies in their purpose and the immune response they aim to achieve, particularly for specific vaccine types like mRNA and viral vector vaccines. For individuals with compromised immune systems, a third dose of an mRNA vaccine (such as Pfizer-BioNTech or Moderna) is often recommended to complete the initial vaccination series. This is because their immune systems may not have mounted a sufficient response after the standard two doses. For example, immunocompromised individuals aged 12 and older are advised to receive an additional dose 28 days after their second shot, ensuring a more robust immune foundation.
In contrast, booster shots are designed to enhance immunity in the general population over time. For mRNA vaccines, a booster is typically administered 5 months after the second dose for individuals aged 12 and older. Viral vector vaccines, like Johnson & Johnson’s Janssen, follow a different schedule: a booster is recommended 2 months after the initial single-dose shot. This difference highlights how vaccine type dictates the timing and necessity of additional doses. Boosters are not just repeats of earlier doses; they are strategically timed to counter waning immunity and emerging variants.
Consider the practical implications: if you received the Janssen vaccine, your booster timeline is significantly shorter than those who received mRNA vaccines. This underscores the importance of knowing your vaccine type and following tailored guidelines. For instance, travelers or those in high-risk environments may prioritize boosters sooner, while immunocompromised individuals must ensure their third dose is properly documented as part of their primary series, not a booster.
A comparative analysis reveals that mRNA vaccines, with their higher efficacy rates, often require boosters to maintain protection against evolving strains like Omicron. Viral vector vaccines, while effective, may necessitate earlier boosters due to their single-dose design. This variation emphasizes the need for personalized vaccine strategies based on individual health status, vaccine type, and community transmission rates. Always consult healthcare providers to determine whether you need a third dose to complete your initial series or a booster to reinforce immunity.
In summary, while both third doses and boosters involve additional shots, their roles differ significantly, especially for mRNA and viral vector vaccines. Understanding these distinctions ensures optimal protection and adherence to public health guidelines. Whether completing your primary series or boosting immunity, the specifics of your vaccine type dictate the path forward.
Is Forte Reserve Bank in Turkey Legitimate? Uncovering the Truth
You may want to see also
Explore related products






![]()
Global Guidelines: Varying recommendations by health organizations (WHO, CDC, EMA)
The World Health Organization (WHO), Centers for Disease Control and Prevention (CDC), and European Medicines Agency (EMA) each approach the question of whether a third vaccine dose and a booster are the same with distinct guidelines, reflecting their unique mandates and regional contexts. WHO, prioritizing global equity, emphasizes that a third dose for immunocompromised individuals is not the same as a booster for the general population. For instance, WHO recommends a third dose of mRNA vaccines (e.g., Pfizer or Moderna) for those with moderate to severe immunocompromise, administered 4 weeks after the second dose, but reserves boosters for high-risk groups in countries with high vaccination rates. This distinction ensures that limited resources are allocated to those most in need, globally.
In contrast, the CDC takes a more population-specific approach, particularly in the context of the U.S. For immunocompromised individuals aged 5 and older, the CDC recommends an additional primary dose 28 days after the second dose of Pfizer or Moderna, followed by a booster at least 3 months later. For the general population, boosters are advised 5 months after the Pfizer or Moderna series or 2 months after Johnson & Johnson. This tiered strategy aims to maximize protection within the U.S. healthcare framework, balancing individual and public health needs.
The EMA, focusing on the European Union, aligns closely with vaccine manufacturers’ data and safety profiles. It defines a booster as a dose given to maintain immunity, distinct from an additional dose needed to achieve full immunity in certain populations. For example, the EMA approves a third dose of Comirnaty (Pfizer) or Spikevax (Moderna) for immunocompromised individuals, while boosters are recommended for all adults 6 months after the primary series. This clarity ensures that member states can implement consistent vaccination strategies based on robust scientific evidence.
These differing recommendations highlight the complexity of global health governance. While WHO advocates for equity, the CDC and EMA tailor their guidelines to regional capacities and epidemiological contexts. For instance, the CDC’s shorter booster interval for Johnson & Johnson recipients reflects its lower initial efficacy compared to mRNA vaccines, a nuance not universally applicable. Practically, travelers and expatriates must navigate these variations, ensuring compliance with both their home country’s and host country’s guidelines.
In summary, while a third dose and booster may serve similar immunological purposes, their definitions and applications vary by organization. WHO’s equity-driven approach, the CDC’s population-specific strategy, and the EMA’s evidence-based framework collectively illustrate the challenges of harmonizing global health recommendations. Individuals should consult local health authorities for precise dosing schedules and eligibility criteria, ensuring optimal protection in their specific context.
Does PNC Bank Charge Monthly Fees? Understanding Account Costs
You may want to see also
Explore related products






![]()
Side Effects: Common reactions and differences between third doses and boosters
Side effects from COVID-19 vaccines are generally mild to moderate and short-lived, but the third dose and booster shots can elicit slightly different reactions. For instance, while both are additional doses administered after the initial series, the third dose is typically given to immunocompromised individuals as part of their primary vaccination to ensure adequate immune response. Boosters, on the other hand, are designed to enhance waning immunity in the general population, often with a lower dosage or a modified formulation. This distinction influences the side effect profile, with boosters sometimes causing more pronounced reactions due to the immune system’s memory response.
Common side effects for both include pain or swelling at the injection site, fatigue, headache, and muscle pain. However, studies suggest that boosters, particularly mRNA-based ones, may lead to more systemic reactions, such as fever or chills, compared to the third dose. For example, a 2022 CDC report noted that 79% of booster recipients reported fatigue, versus 68% after the third dose in immunocompromised individuals. This difference is attributed to the immune system’s heightened recognition of the antigen in booster recipients, triggering a more vigorous response.
Age and health status also play a role in side effect severity. Younger individuals (18–40 years) tend to experience more intense reactions to boosters, while older adults (65+) may have milder symptoms due to age-related immune changes. Immunocompromised individuals, who often receive a third dose, may experience fewer side effects due to their suppressed immune response, though this varies based on the degree of immunosuppression. Practical tips include scheduling boosters or third doses on a day when rest is possible and using over-the-counter pain relievers like acetaminophen or ibuprofen to manage discomfort.
A comparative analysis reveals that while both doses serve to strengthen immunity, the booster’s purpose of reinvigorating memory cells can lead to a more noticeable reaction. For instance, the Pfizer-BioNTech booster (30 µg) is half the dose of the primary series but still elicits robust side effects in many recipients. In contrast, the third dose for immunocompromised individuals (often a full dose) is less likely to cause severe reactions due to their baseline immune status. Understanding these differences helps individuals prepare for what to expect and underscores the importance of personalized vaccination strategies.
In conclusion, while side effects from third doses and boosters overlap, boosters often provoke more pronounced reactions due to their immunological purpose. Tailoring expectations based on age, health, and dose type can alleviate concerns and encourage adherence to vaccination schedules. Monitoring symptoms and following post-vaccination guidelines remain crucial for a smooth experience.
N26's US Banking Partner: Unveiling the Financial Institution Behind the App
You may want to see also
Frequently asked questions
Not always. A 3rd dose is typically given to individuals with weakened immune systems to complete their initial vaccination series, while a booster is administered to the general population to enhance immunity over time.
No, immunocompromised individuals usually need a 3rd dose as part of their primary series, followed by a booster later to further strengthen protection.
In some cases, yes. For example, Pfizer and Moderna boosters are often given at a lower dose than the primary series doses, while a 3rd dose for immunocompromised individuals is typically a full dose.
It depends on your health status and vaccine guidelines. Immunocompromised individuals may need both, while others may only need a booster after completing their primary series.
The timing varies by vaccine and health status. For immunocompromised individuals, a booster is often recommended 3-6 months after the 3rd dose, but consult healthcare providers for specific guidance.