The efficacy of a vaccine is a critical measure of its ability to prevent disease in a population, and a 66% efficacy rate, while not as high as some vaccines like those for measles or polio, is still considered good in many contexts. This level of efficacy means that, on average, the vaccine reduces the risk of disease by 66% in vaccinated individuals compared to those who are unvaccinated. For example, vaccines with similar efficacy rates, such as the flu vaccine, are widely used and play a significant role in public health by reducing hospitalizations and severe outcomes. However, the perception of whether 66% is good can depend on the specific disease, its severity, and the availability of other preventive measures. In the case of COVID-19 vaccines, for instance, a 66% efficacy rate has been shown to substantially decrease hospitalizations and deaths, making it a valuable tool in combating the pandemic. Ultimately, the effectiveness of a vaccine must be evaluated alongside its safety profile, the burden of the disease it prevents, and the broader public health goals it aims to achieve.
| Characteristics | Values |
|---|---|
| Efficacy Definition | Percentage reduction in disease incidence in vaccinated group vs. placebo. |
| 66% Efficacy Context | Considered "good" but not "excellent" compared to vaccines like COVID-19 mRNA vaccines (90-95%). |
| FDA Approval Threshold | ≥50% efficacy for pandemic vaccines (e.g., flu vaccines often have 40-60% efficacy). |
| Public Health Impact | Still provides substantial benefit by reducing severe disease, hospitalizations, and deaths. |
| Examples of 66% Efficacy Vaccines | Some influenza vaccines, certain COVID-19 vaccines (e.g., Sinovac's CoronaVac in some studies). |
| Comparison to Other Vaccines | Lower than mRNA COVID-19 vaccines (90-95%) but higher than some flu vaccines (40-60%). |
| Real-World Effectiveness | May vary due to factors like virus variants, population immunity, and adherence. |
| Expert Opinion | Generally viewed as acceptable, especially in contexts of limited alternatives or urgent need. |
| Global Health Perspective | Valuable in low-resource settings or during outbreaks where higher-efficacy vaccines are unavailable. |
| Limitations | May require booster doses or additional measures for optimal protection. |
Explore related products

$10.89 $32.95





What You'll Learn
![]()
Historical Vaccine Efficacy Rates
Vaccine efficacy rates have historically varied widely, reflecting the complexity of the diseases they target and the technologies available at the time. For instance, the smallpox vaccine, one of the earliest successes, demonstrated an efficacy of approximately 95%, leading to the global eradication of the disease in 1980. This high rate was critical, as smallpox had a mortality rate of up to 30%. In contrast, the annual influenza vaccine typically ranges between 40% and 60% efficacy due to the virus’s rapid mutation and the need to predict dominant strains months in advance. These examples highlight how historical efficacy rates are shaped by both the pathogen’s characteristics and the vaccine’s design.
Analyzing historical data reveals that a 66% efficacy rate falls into a middle ground, often sufficient for public health impact but not ideal for individual protection. The polio vaccine, for example, achieved 90% efficacy with its inactivated (IPV) form and even higher with the oral (OPV) version, contributing to a 99% global reduction in cases since 1988. Conversely, the typhoid vaccine offers around 50-80% protection, depending on the formulation, yet it remains a vital tool in endemic regions. A 66% efficacy rate, while not groundbreaking, can still significantly reduce disease burden when combined with high vaccination coverage, as seen in measles vaccines, which require at least 90% population immunity to prevent outbreaks but have individual efficacy rates around 93% after two doses.
Instructively, understanding historical efficacy rates helps set realistic expectations for new vaccines. The measles vaccine’s success relied on its high efficacy and widespread administration, typically starting at 12 months of age with a second dose at 4-6 years. For vaccines with lower efficacy, such as the malaria vaccine (RTS,S, with ~30-50% efficacy), strategies like combining vaccination with other interventions (e.g., bed nets) become essential. Similarly, a 66% efficacy rate might necessitate booster doses or targeted distribution to high-risk groups, as seen with the shingles vaccine (Shingrix), which achieves over 90% efficacy in adults over 50 after two doses spaced 2-6 months apart.
Persuasively, historical context underscores that even moderately efficacious vaccines can transform public health. The pertussis (whooping cough) vaccine, with ~80-85% efficacy, has drastically reduced infant mortality since its introduction in the 1940s, despite waning immunity over time. A 66% efficacy rate, while not optimal, can still prevent severe outcomes and hospitalizations, as evidenced by the COVID-19 vaccines during the pandemic. For example, the AstraZeneca vaccine, with ~66-70% efficacy against symptomatic disease, played a pivotal role in curbing hospitalizations and deaths, particularly in resource-limited settings. This reinforces the value of imperfect vaccines in controlling disease spread.
Comparatively, historical efficacy rates also illustrate the trade-offs between speed, safety, and effectiveness. The mumps vaccine, part of the MMR series, has ~75-85% efficacy after one dose and ~88% after two, yet outbreaks still occur in undervaccinated communities. Similarly, the rotavirus vaccine, with ~85-98% efficacy in developed countries but ~50-60% in low-income regions, highlights how efficacy can vary by population. A 66% efficacy rate, while modest, can be a starting point for improvement, as seen with the HPV vaccine, which initially had ~70% efficacy against certain strains but now offers ~90% protection with newer formulations. This evolution demonstrates the potential for refining vaccines over time.
Does Your Bank Verify Your Employer? What You Need to Know
You may want to see also
Explore related products






![]()
Comparing COVID-19 Vaccine Efficacies
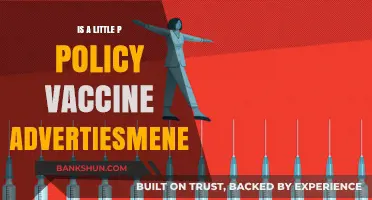
A 66% efficacy rate for a vaccine might initially seem underwhelming, especially when compared to the near-perfect protection offered by childhood vaccines like measles (97%). However, this figure takes on new meaning when examining the specific context of COVID-19 vaccines.
Efficacy rates are calculated based on clinical trials, where vaccinated and unvaccinated groups are compared to see who develops the disease. A 66% efficacy means that in these trials, vaccinated individuals were 66% less likely to contract COVID-19 compared to those receiving a placebo. This doesn't mean the vaccine is only partially effective; it signifies a substantial reduction in risk.
Consider the real-world implications. A vaccine with 66% efficacy can significantly curb transmission and prevent severe illness, even if it doesn't completely eliminate the possibility of infection. For instance, the AstraZeneca vaccine, with an efficacy of around 66-70%, has been instrumental in protecting millions worldwide, particularly in low- and middle-income countries. Its impact extends beyond individual protection, contributing to herd immunity and reducing the strain on healthcare systems.
This highlights a crucial point: vaccine efficacy is just one factor to consider. Other aspects like accessibility, cost, and ease of distribution play vital roles in a vaccine's overall effectiveness in combating a global pandemic.
When comparing COVID-19 vaccine efficacies, it's essential to understand the nuances. The Pfizer-BioNTech and Moderna mRNA vaccines boast higher efficacies, around 94-95%, but require ultra-cold storage, making distribution challenging in certain regions. The Johnson & Johnson vaccine, with a slightly lower efficacy of around 66%, offers the advantage of a single dose and standard refrigeration, making it more accessible in resource-limited settings.
Ultimately, a 66% efficacy for a COVID-19 vaccine is not merely "good" – it's a powerful tool in our arsenal against a devastating pandemic. It represents a significant reduction in risk, contributes to herd immunity, and offers practical advantages in terms of distribution. While higher efficacy rates are desirable, the real-world impact of a vaccine extends far beyond a single number. It's about accessibility, practicality, and the collective effort to protect global health.
Step-by-Step Guide to Registering for GTB Internet Banking Easily
You may want to see also
Explore related products






![]()
Public Health Impact of 66%
A vaccine with 66% efficacy might seem underwhelming compared to the 95% benchmarks set by mRNA COVID-19 vaccines, but its public health impact hinges on context, not just numbers. Consider influenza vaccines, which typically range from 40-60% efficacy yet remain cornerstone tools in seasonal flu prevention. The difference? Influenza’s lower transmission rate and less severe outcomes in most populations allow even moderately effective vaccines to significantly reduce hospitalizations and deaths. A 66% effective vaccine in a highly contagious disease like measles, however, would fall short of herd immunity thresholds (90-95%), risking outbreaks. Efficacy alone is insufficient—disease severity, transmission dynamics, and population immunity must shape expectations.
To maximize the public health impact of a 66% effective vaccine, targeted deployment strategies are critical. For instance, prioritizing high-risk groups (elderly, immunocompromised, or those in crowded settings) can amplify benefits. During the 2009 H1N1 pandemic, vaccines with ~60% efficacy were strategically distributed to healthcare workers and pregnant women, curbing severe cases despite limited overall supply. Pairing vaccination with non-pharmaceutical interventions (masking, ventilation) creates a layered defense, compensating for lower efficacy. For a respiratory virus, this could mean mandating masks in schools during peak seasons or improving air filtration in nursing homes—practical steps that bridge the efficacy gap.
Critics often overlook the logistical advantages of moderately effective vaccines. A 66% efficacy vaccine with simpler storage requirements (e.g., fridge-stable vs. ultra-cold chain) or fewer doses (one vs. two) could reach more people faster, particularly in low-resource settings. For example, the Johnson & Johnson COVID-19 vaccine (66% efficacy against infection, 85% against severe disease) played a pivotal role in hard-to-reach populations due to its single-dose regimen. Public health officials must weigh these trade-offs: higher efficacy vs. accessibility. A vaccine that’s 66% effective but widely adopted may outperform a 90% vaccine with limited uptake due to cost, hesitancy, or distribution barriers.
Finally, the long-term impact of a 66% effective vaccine depends on its ability to adapt to evolving pathogens. Viral mutations can erode efficacy over time, as seen with seasonal flu vaccines. However, a vaccine that reduces severe outcomes (hospitalization, death) even at 66% efficacy remains a public health win, as it eases strain on healthcare systems. For instance, a dengue vaccine with ~60% efficacy against symptomatic disease has been deployed in endemic regions, not to eliminate the virus, but to prevent hemorrhagic fever—a life-threatening complication. The takeaway? A 66% efficacy vaccine isn’t inherently “good” or “bad”—its value lies in how it’s tailored to the disease, population, and practical realities of implementation.
Cayman Islands Banks: IRS Reporting and You
You may want to see also
Explore related products






![]()
Factors Affecting Vaccine Efficacy
Vaccine efficacy is a critical metric, but it’s not a static number. A 66% efficacy rate, for instance, doesn’t tell the whole story. To understand its value, consider the factors that influence how well a vaccine performs in the real world. These factors range from biological to logistical, each playing a unique role in shaping the final efficacy figure. Let’s break them down.
Biological Variability: The Human Factor
Individual immune responses differ dramatically based on age, genetics, and underlying health conditions. For example, older adults often mount weaker immune responses due to immunosenescence, which can reduce vaccine efficacy. A 66% efficacy rate might reflect this variability, as the vaccine performs differently across age groups. Similarly, chronic illnesses like diabetes or HIV can impair immune function, lowering the vaccine’s effectiveness. Manufacturers often address this by adjusting dosages—such as higher antigen concentrations for older adults—or recommending booster shots to enhance immunity.
Pathogen Evolution: The Moving Target
Viruses and bacteria mutate over time, potentially reducing vaccine efficacy. For instance, influenza vaccines typically range from 40–60% efficacy due to rapid viral evolution. A 66% efficacy rate might indicate a vaccine’s performance against a dominant strain but could drop if new variants emerge. mRNA vaccines, like those for COVID-19, offer flexibility here, as their design allows for rapid updates to target new variants. However, this requires global surveillance systems to detect changes promptly and regulatory frameworks to expedite approvals.
Logistical Challenges: The Last Mile
Even the most effective vaccine can falter if not administered correctly. Storage, handling, and adherence to dosing schedules are critical. For example, vaccines requiring ultra-cold storage (e.g., -70°C for Pfizer’s COVID-19 vaccine) face distribution hurdles in low-resource settings, potentially compromising efficacy. Similarly, missing a booster dose can significantly reduce protection. A 66% efficacy rate might reflect real-world challenges rather than the vaccine’s inherent limitations. Practical solutions include investing in cold chain infrastructure and simplifying dosing regimens to improve compliance.
Study Design: The Numbers Game
Efficacy rates are derived from clinical trials, which vary in design and population. A trial conducted in a high-transmission setting might report lower efficacy than one in a controlled environment. For instance, a vaccine tested during a surge of infections could show 66% efficacy, while the same vaccine might perform better in a less exposed population. Trial duration also matters; short-term studies may overestimate efficacy if long-term immunity wanes. Understanding these nuances is crucial for interpreting efficacy data and setting realistic expectations.
In conclusion, a 66% efficacy rate isn’t inherently good or bad—it’s a snapshot influenced by biological, logistical, and methodological factors. By addressing these variables, we can maximize a vaccine’s real-world impact, ensuring that even modest efficacy translates to meaningful protection.
Mastering Gold Banking in Aura Kingdom: Essential Tips and Strategies
You may want to see also
Explore related products






![]()
66% vs. Herd Immunity Thresholds
A vaccine's efficacy of 66% might initially seem underwhelming, especially when compared to the high bars set by vaccines like measles (97%) or polio (99%). However, the story becomes more nuanced when considering herd immunity thresholds (HITs), the vaccination coverage needed to interrupt disease spread. For diseases like measles, the HIT is around 95%, meaning 66% efficacy would fall short even with full population coverage. But for diseases with lower transmissibility, such as influenza (HIT ~60-70%), a 66% efficacious vaccine could still play a pivotal role in achieving herd immunity, especially when combined with other public health measures.
To understand the practical implications, consider a hypothetical respiratory virus with an HIT of 80%. If a 66% efficacious vaccine is administered to 90% of the population, the effective coverage would be approximately 60% (0.66 * 0.90). While this falls below the HIT, it significantly reduces disease transmission, lowering infection rates and protecting vulnerable populations. For instance, in a population of 1 million, this scenario could prevent hundreds of thousands of cases, hospitalizations, and deaths, particularly among the elderly or immunocompromised.
However, achieving herd immunity with a 66% efficacious vaccine requires meticulous planning. Vaccination campaigns must prioritize high-risk groups, such as healthcare workers and those over 65, to maximize impact. Additionally, booster doses may be necessary to maintain immunity, as seen with COVID-19 vaccines. For example, a two-dose regimen with a 66% efficacy vaccine could be supplemented by a booster after six months, potentially raising the effective protection to levels closer to the HIT.
Critics argue that relying on a 66% efficacious vaccine for herd immunity is risky, as it leaves gaps in protection that could allow outbreaks. Yet, real-world examples, like the use of influenza vaccines, demonstrate that even moderately efficacious vaccines can substantially reduce disease burden when paired with high uptake rates. For instance, during the 2019-2020 flu season, a vaccine with 39% efficacy prevented an estimated 7.52 million illnesses and 6,300 deaths in the U.S. alone.
In conclusion, while 66% efficacy may not be ideal, it is not insignificant, especially when aligned with diseases having lower HITs. Public health strategies must focus on maximizing vaccine coverage, targeting vulnerable populations, and potentially incorporating boosters to bridge the gap between efficacy and herd immunity. By doing so, even a vaccine with moderate efficacy can become a powerful tool in controlling disease spread.
How to Cancel a Transaction in Axis Bank: Step-by-Step Guide
You may want to see also
Frequently asked questions
Yes, 66% efficacy is considered good for a vaccine, as it indicates that the vaccine reduces the risk of disease by 66% compared to those who are unvaccinated.
A 66% efficacy is lower than some vaccines like the measles vaccine (97%) but still higher than others like the flu vaccine (40-60%). It is still effective in preventing illness and reducing severity.
No, a 66% efficacy means the vaccine still provides significant protection against the disease, reduces hospitalizations, and saves lives, making it worthwhile.
While a 66% efficacy vaccine may not completely stop the spread, it can significantly reduce transmission by lowering the number of infections and severe cases.
Vaccine efficacy varies based on factors like the disease, the immune response it triggers, and the population studied. Some diseases are easier to target with vaccines than others.