The question of whether a TB test is a live vaccine often arises due to confusion between the tuberculin skin test (TST) and the Bacille Calmette-Guérin (BCG) vaccine. The TST, commonly known as the PPD test, is not a vaccine but rather a diagnostic tool used to detect latent tuberculosis infection by measuring the immune system’s response to TB antigens. In contrast, the BCG vaccine is a live attenuated vaccine administered to prevent severe forms of TB, particularly in infants and young children in high-risk regions. Understanding the distinction between these two is crucial, as the TST does not confer immunity, while the BCG vaccine provides partial protection against TB but does not prevent latent infection.
| Characteristics | Values |
|---|---|
| Type of TB Test | There are two main types of TB tests: the Tuberculin Skin Test (TST) and the Interferon-Gamma Release Assay (IGRA) blood test. Neither of these tests is a vaccine. |
| Live Vaccine | No, the TB tests (TST and IGRA) are not live vaccines. They do not contain any live bacteria or viruses. |
| Purpose | The TB tests are used to detect if a person has been infected with Mycobacterium tuberculosis, the bacteria that causes tuberculosis (TB). They do not provide immunity or protection against TB. |
| TST (Mantoux Test) | Involves injecting a small amount of a substance called PPD tuberculin just under the skin on the forearm. A positive reaction (hard, raised bump) usually indicates TB infection. |
| IGRA Blood Test | Measures the immune system’s response to TB bacteria by detecting the release of interferon-gamma when white blood cells are exposed to TB antigens in a lab setting. |
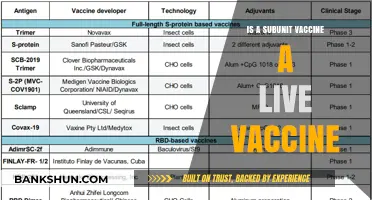
| Vaccine for TB | The Bacille Calmette-Guérin (BCG) vaccine is a live attenuated vaccine used in some countries to protect against severe forms of TB, particularly in children. It is not used for testing TB infection. |
| Confusion | The confusion may arise because the BCG vaccine can cause a positive TST result, but the TST itself is not a vaccine. |
| Latest Data (as of 2023) | No changes in the classification of TB tests as non-vaccine tools. BCG remains the only live vaccine for TB prevention in specific populations. |
Explore related products






What You'll Learn
- TB Test Types: Differentiating between live and non-live vaccines used in TB testing
- TST vs. IGRA: Comparing Tuberculin Skin Test and Interferon-Gamma Release Assay methods
- BCG Vaccine: Understanding if the BCG vaccine is live and its relation to TB tests
- Live Vaccine Risks: Potential risks of live vaccines in immunocompromised individuals during TB testing
- False Positives: How live vaccines like BCG can cause false-positive TB test results
![]()
TB Test Types: Differentiating between live and non-live vaccines used in TB testing
Tuberculosis (TB) testing relies on two primary methods: the Tuberculin Skin Test (TST) and the Interferon-Gamma Release Assay (IGRA). Neither of these tests uses a live vaccine. Instead, they assess the immune system’s response to TB antigens. The TST, also known as the Mantoux test, involves injecting a small amount of purified protein derivative (PPD) from the TB bacterium just beneath the skin. A positive reaction, indicated by a raised, hardened area at the injection site, suggests prior exposure to TB. The IGRA, a blood test, measures the release of interferon-gamma when white blood cells are exposed to TB-specific antigens. Both tests are non-invasive and do not introduce live TB bacteria, making them safe for individuals with weakened immune systems.
The confusion about live vaccines in TB testing often stems from the Bacille Calmette-Guérin (BCG) vaccine, which *is* a live attenuated vaccine used for TB prevention, not testing. Administered primarily to infants in high-burden countries, the BCG vaccine contains a weakened strain of *Mycobacterium bovis*. While it can cause a false-positive result in the TST, it does not interfere with IGRA results, as the latter targets antigens not present in the BCG vaccine. This distinction highlights the importance of choosing the appropriate test based on vaccination history and risk factors. For instance, healthcare workers in the U.S. often prefer IGRA over TST due to its accuracy in BCG-vaccinated individuals.
When deciding between TST and IGRA, consider practical factors such as cost, convenience, and patient age. The TST requires two visits—one for administration and another 48–72 hours later for reading—while IGRA needs only a single blood draw. TST is more cost-effective but may be less reliable in children under 5 or immunocompromised individuals. IGRA, though pricier, offers greater specificity and is not influenced by prior BCG vaccination. For example, a 30-year-old immigrant from a high-TB-prevalence country with a history of BCG vaccination would benefit more from an IGRA test to avoid false-positive results.
A critical takeaway is that neither TB test type involves live vaccines, but understanding their differences ensures accurate diagnosis and appropriate follow-up. For instance, a positive TST or IGRA does not confirm active TB disease—it indicates latent TB infection, requiring further chest X-rays or sputum tests. Always consult healthcare guidelines, such as those from the CDC, to determine the best testing approach. By differentiating between live vaccines like BCG and non-live testing methods, patients and providers can navigate TB screening with clarity and confidence.
Does M&T Bank Offer Coin Counting Services? Find Out Here
You may want to see also
Explore related products






![]()
TST vs. IGRA: Comparing Tuberculin Skin Test and Interferon-Gamma Release Assay methods
The Tuberculin Skin Test (TST), also known as the Mantoux test, has been a cornerstone of tuberculosis (TB) diagnosis for over a century. It involves injecting a small amount of purified protein derivative (PPD) from the TB bacterium just beneath the skin, typically on the forearm. After 48 to 72 hours, a trained healthcare provider measures the size of the induration (hardened, raised area) to determine if the test is positive. A positive TST indicates exposure to *Mycobacterium tuberculosis*, but it does not differentiate between latent TB infection (LTBI) and active TB disease. Importantly, the TST is not a live vaccine; it does not contain live bacteria and cannot cause TB. However, its accuracy can be influenced by factors such as prior Bacille Calmette-Guérin (BCG) vaccination, which can lead to false-positive results, especially in individuals vaccinated after infancy.
In contrast, the Interferon-Gamma Release Assay (IGRA) is a blood-based test that measures the immune system’s response to TB-specific antigens. Unlike the TST, IGRA does not require a second visit for result interpretation, making it more convenient for patients. Two FDA-approved IGRA tests are available: QuantiFERON-TB Gold Plus and T-SPOT.TB. Both tests detect the release of interferon-gamma by T-cells in response to TB antigens. IGRA is less affected by prior BCG vaccination, making it a preferred option in BCG-vaccinated populations. However, it is not without limitations; IGRA can yield indeterminate results if the immune response is compromised, such as in individuals with HIV or those on immunosuppressive therapy. Additionally, IGRA is generally more expensive than TST, which can influence its accessibility in resource-limited settings.
When comparing TST and IGRA, the choice of test depends on several factors, including patient history, BCG vaccination status, and logistical considerations. For instance, TST may be more practical in pediatric populations, as it requires only a skin injection and no blood draw. However, IGRA is often favored for adults, particularly those with a history of BCG vaccination or those at risk of anergy (reduced immune response), such as the elderly or immunocompromised individuals. Both tests have their place in TB diagnostics, but neither can definitively diagnose active TB disease; additional tests like chest X-rays or sputum cultures are required for confirmation.
Practical tips for administering these tests include ensuring proper training for TST placement and reading, as misinterpretation of induration size can lead to false results. For IGRA, timely processing of blood samples is critical, as delays can affect the accuracy of the test. Patients should be informed about the limitations of both tests, such as the inability to distinguish between LTBI and active TB, and the potential for false results due to factors like prior BCG vaccination or immune status. Ultimately, the decision between TST and IGRA should be guided by clinical context, patient characteristics, and available resources.
In conclusion, while neither TST nor IGRA is a live vaccine, their roles in TB diagnostics are distinct yet complementary. TST remains a cost-effective and widely accessible option, particularly in settings with limited resources, while IGRA offers advantages in specificity and convenience, especially in BCG-vaccinated populations. Understanding the strengths and limitations of each method is essential for accurate TB screening and management.
Master Monopoly Ultimate Banking: A Step-by-Step Setup Guide
You may want to see also
Explore related products





![]()
BCG Vaccine: Understanding if the BCG vaccine is live and its relation to TB tests
The BCG vaccine, a cornerstone in the fight against tuberculosis (TB), is indeed a live attenuated vaccine. This means it contains a weakened but still living form of the *Mycobacterium baculli Calmette-Guérin* (BCG) bacterium. Unlike inactivated or subunit vaccines, which use dead pathogens or their components, the BCG vaccine introduces a live organism into the body to stimulate a robust immune response. This live nature is both its strength and a consideration for certain populations, such as immunocompromised individuals, for whom it may pose risks.
Understanding the BCG vaccine’s live status is crucial when discussing its relation to TB tests, particularly the tuberculin skin test (TST) and interferon-gamma release assays (IGRAs). The TST, also known as the Mantoux test, involves injecting a small amount of purified protein derivative (PPD) from the TB bacterium into the skin. A positive reaction—indicated by swelling at the injection site—suggests exposure to TB or prior BCG vaccination. Because the BCG vaccine uses a live, albeit attenuated, mycobacterium, it can cause false-positive results in the TST, complicating the interpretation of TB exposure. This overlap highlights the importance of considering vaccination history when administering and interpreting TB tests.
In contrast, IGRAs, such as the QuantiFERON-TB Gold test, measure the immune system’s response to TB-specific antigens by analyzing blood samples. These tests are less likely to be affected by prior BCG vaccination, making them a preferred option in BCG-vaccinated populations. However, IGRAs are not without limitations; they require specialized equipment and are more expensive than the TST. For healthcare providers, understanding the interplay between the BCG vaccine’s live nature and TB testing methods is essential for accurate diagnosis and treatment planning.
Practical considerations arise when administering the BCG vaccine, typically given as a single dose of 0.05 mL via intradermal injection, usually in the upper arm, to infants and children in high-TB-burden countries. In low-incidence regions, it is often reserved for high-risk groups, such as healthcare workers or those with known TB exposure. For individuals who have received the BCG vaccine, it’s advisable to inform healthcare providers before undergoing TB testing to ensure accurate interpretation of results. Additionally, while the BCG vaccine provides moderate protection against severe forms of TB in children, its efficacy against pulmonary TB in adults is variable, underscoring the need for complementary preventive measures.
In summary, the BCG vaccine’s live attenuated nature is a double-edged sword: it offers significant protection against severe TB, particularly in children, but can complicate TB test results. Healthcare providers must weigh these factors when deciding on vaccination and testing strategies, especially in populations with varying TB prevalence. By understanding this relationship, individuals and clinicians can navigate TB prevention and diagnosis more effectively, ensuring timely and accurate interventions.
Highland Indiana: How Far Is It?
You may want to see also
Explore related products






![]()
Live Vaccine Risks: Potential risks of live vaccines in immunocompromised individuals during TB testing
Live vaccines, such as the Bacille Calmette-Guérin (BCG) vaccine used in some tuberculosis (TB) testing and prevention protocols, contain weakened but still active pathogens. While generally safe for healthy individuals, these vaccines pose unique risks to immunocompromised populations. Unlike inactivated vaccines, live vaccines replicate within the body, relying on a functional immune system to control their growth. In individuals with weakened immunity—due to conditions like HIV, cancer treatments, or organ transplants—this replication can lead to uncontrolled vaccine-strain infections, a condition known as vaccine-associated disease. For instance, BCG vaccination in severely immunocompromised patients has been linked to disseminated BCG infection, a rare but serious complication characterized by systemic symptoms and organ involvement.
Consider the case of a 10-year-old child with leukemia undergoing chemotherapy. Despite being in a high-risk TB exposure group, administering the BCG vaccine could be life-threatening due to their compromised immune state. The U.S. Centers for Disease Control and Prevention (CDC) explicitly advises against BCG vaccination for individuals with severe immunodeficiency, emphasizing the potential for the vaccine strain to cause severe, even fatal, disease. Similarly, immunocompromised adults, such as those on high-dose corticosteroids or biologic therapies, face heightened risks if inadvertently exposed to live vaccines during TB testing or prevention efforts.
The Mantoux tuberculin skin test (TST) and interferon-gamma release assays (IGRAs) are alternative TB diagnostic tools that do not involve live vaccines, making them safer options for immunocompromised individuals. However, confusion arises when the BCG vaccine is mistakenly considered a diagnostic tool rather than a preventive measure. Healthcare providers must carefully assess a patient’s immune status before recommending any TB-related intervention. For example, a 45-year-old patient with rheumatoid arthritis on methotrexate and prednisone should avoid BCG vaccination but can safely undergo TST or IGRA testing to evaluate latent TB infection.
Practical precautions include screening for immunocompromising conditions before administering live vaccines and prioritizing non-live diagnostic methods for at-risk populations. Patients should disclose all medications, underlying illnesses, and recent treatments to their healthcare provider. For instance, a 60-year-old organ transplant recipient on immunosuppressive therapy should never receive BCG, even in TB-endemic regions, due to the risk of vaccine-induced complications. Instead, focus should shift to environmental TB exposure reduction and close monitoring for active disease symptoms.
In summary, while live vaccines like BCG play a critical role in TB prevention, their use in immunocompromised individuals demands extreme caution. Missteps can lead to severe, preventable complications. Healthcare providers must differentiate between preventive and diagnostic TB tools, prioritize patient immune status assessments, and adhere to guidelines that safeguard vulnerable populations. By doing so, they can mitigate risks while addressing TB concerns effectively.
Barn Home Financing: Local Bank Options Explored
You may want to see also
Explore related products






![]()
False Positives: How live vaccines like BCG can cause false-positive TB test results
The Bacille Calmette-Guerin (BCG) vaccine, a live attenuated tuberculosis (TB) vaccine, has been administered to over 4 billion individuals worldwide, primarily to infants in high-burden countries. While its efficacy in preventing severe TB in children is well-documented, a lesser-known consequence is its potential to cause false-positive results in TB skin tests (TST) and interferon-gamma release assays (IGRAs). This phenomenon occurs because the BCG vaccine contains a live, but weakened, strain of *Mycobacterium bovis*, which shares antigenic similarities with *Mycobacterium tuberculosis*. When a vaccinated individual undergoes TB testing, their immune system may react to these shared antigens, triggering a positive result even in the absence of active TB infection.
Consider the TST, where a small amount of purified protein derivative (PPD) is injected intradermally. In BCG-vaccinated individuals, the resulting induration size—typically measured 48–72 hours post-test—can exceed the 10 mm threshold for a positive result, particularly in those vaccinated within the past 10 years. For instance, a study in *Vaccine* (2018) found that 40% of BCG-vaccinated adolescents exhibited false-positive TST results, compared to 10% in the unvaccinated group. Similarly, IGRAs, which measure T-cell release of interferon-gamma in response to TB-specific antigens, can also yield false positives in BCG-vaccinated individuals, though this is less common due to the test’s specificity for *M. tuberculosis* antigens.
Clinicians must interpret TB test results cautiously in BCG-vaccinated populations, especially in countries with high vaccination coverage. For example, in Brazil, where BCG is universally administered at birth, relying solely on TST for TB screening could lead to unnecessary treatments with isoniazid, a first-line TB drug with potential hepatotoxic side effects. To mitigate this, the CDC recommends using a higher cutoff for TST induration size (15 mm) in BCG-vaccinated individuals or prioritizing IGRAs, which are less affected by BCG vaccination. However, IGRAs are not without limitations; they require specialized equipment and are cost-prohibitive in resource-limited settings.
A practical approach involves obtaining a detailed vaccination history and considering epidemiological risk factors, such as recent TB exposure or immunosuppression. For instance, a 25-year-old BCG-vaccinated immigrant from a high-burden country with a 12 mm TST induration and no TB symptoms might warrant repeat testing or IGRA confirmation before initiating treatment. Conversely, a symptomatic individual with a positive IGRA result should be evaluated for active TB regardless of BCG status. This tailored strategy balances the need for accurate diagnosis with the practical realities of TB testing in diverse populations.
In conclusion, while the BCG vaccine remains a cornerstone of TB prevention, its impact on TB test results underscores the importance of context-specific interpretation. By understanding the mechanisms of false positives and adopting a nuanced approach to testing, healthcare providers can avoid misdiagnosis and ensure appropriate care for at-risk individuals. This is particularly critical in global health settings, where the interplay between vaccination policies and diagnostic accuracy shapes TB control efforts.
Generate Your Axis Bank Telebanking PIN: A Step-by-Step Guide
You may want to see also
Frequently asked questions
No, a TB test, specifically the Tuberculin Skin Test (TST) or the Interferon-Gamma Release Assay (IGRA), is not a vaccine. It is a diagnostic tool used to detect if someone has been infected with tuberculosis (TB).
No, the TB test does not contain live bacteria. The TST uses a purified protein derivative (PPD) from the TB bacterium, while the IGRA is a blood test that measures the immune response to TB antigens.
No, the TB test cannot give you tuberculosis. It is a safe diagnostic procedure that does not introduce live TB bacteria into the body.
No, the BCG vaccine is a live attenuated vaccine used to protect against severe forms of TB, particularly in children. It is not a test for TB infection but rather a preventive measure. A TB test is a separate diagnostic tool.