The spike protein has become a focal point in discussions surrounding COVID-19 vaccines, as it plays a critical role in both the virus's ability to infect cells and the immune response triggered by vaccination. The spike protein is a key component of the SARS-CoV-2 virus, enabling it to attach to and enter human cells. COVID-19 vaccines, such as those developed by Pfizer-BioNTech and Moderna, utilize mRNA technology to instruct cells to produce a harmless version of this spike protein, prompting the immune system to recognize and combat it. This process generates antibodies and immune memory, providing protection against severe illness if exposed to the actual virus. Despite concerns and misinformation, the spike protein in vaccines is safe, temporary, and essential for inducing immunity without causing COVID-19 infection. Understanding its role clarifies how vaccines effectively protect against the virus while dispelling myths about their safety and efficacy.
| Characteristics | Values |
|---|---|
| Presence in Vaccines | Yes, the spike protein or its components are included in COVID-19 vaccines (e.g., mRNA vaccines like Pfizer-BioNTech and Moderna, viral vector vaccines like AstraZeneca and Johnson & Johnson). |
| Purpose | To induce an immune response by mimicking the SARS-CoV-2 virus's spike protein, enabling the body to recognize and fight the virus. |
| Type in mRNA Vaccines | Encoded as mRNA, instructing cells to produce the spike protein temporarily. |
| Type in Viral Vector Vaccines | Delivered via a harmless virus (vector) that introduces the spike protein gene into cells. |
| Stability | Stabilized in a prefusion conformation (e.g., through mutations like K986P and V987P) to enhance immune response. |
| Immunogenicity | Highly immunogenic, eliciting neutralizing antibodies and T-cell responses. |
| Safety | Extensive clinical trials confirm safety; rare side effects (e.g., myocarditis in young males) are closely monitored. |
| Duration in Body | Transient; mRNA degrades within days, and spike protein is cleared within weeks. |
| Shedding | No evidence of spike protein shedding or transmission from vaccinated individuals. |
| Variants | Vaccines target the original spike protein, but updated formulations (e.g., bivalent boosters) include variants like Omicron. |
| Allergenicity | Rare allergic reactions (e.g., anaphylaxis) reported but manageable with medical supervision. |
| Long-Term Effects | No long-term adverse effects related to the spike protein have been identified in studies. |
Explore related products






What You'll Learn
- Spike Protein Function: Role in COVID-19 infection and vaccine-induced immunity
- Vaccine Design: How mRNA and viral vector vaccines encode spike proteins
- Safety Concerns: Addressing myths about spike protein toxicity or side effects
- Immune Response: How the body recognizes and responds to the spike protein
- Variants and Efficacy: Impact of spike protein mutations on vaccine effectiveness
![]()
Spike Protein Function: Role in COVID-19 infection and vaccine-induced immunity
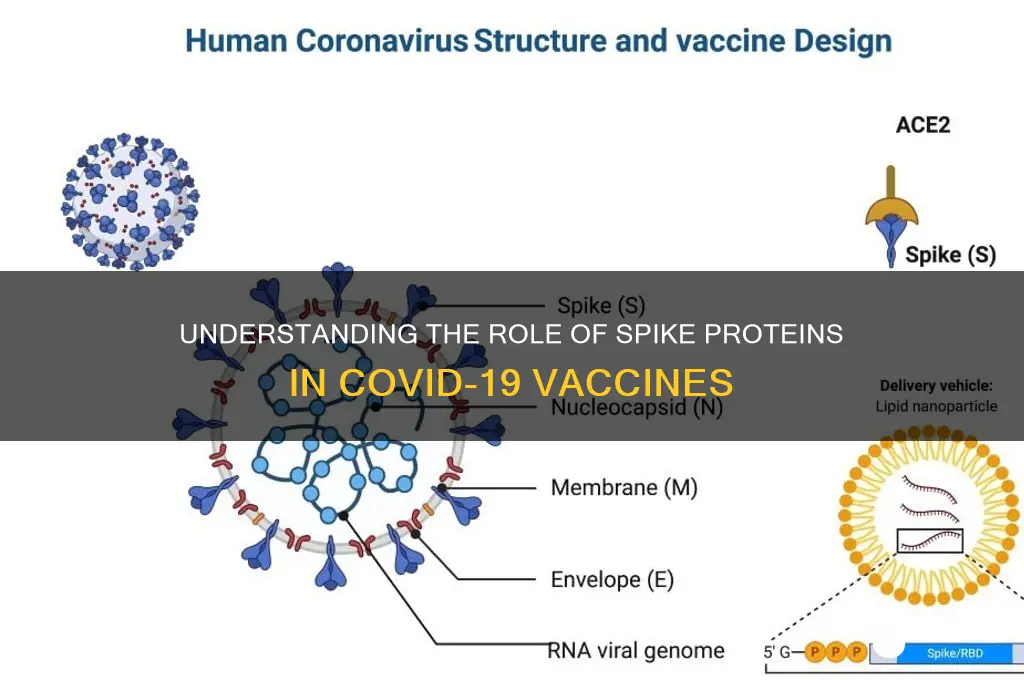
The spike protein is the key to SARS-CoV-2's ability to infiltrate human cells. This club-shaped protein, protruding from the virus's surface, binds to ACE2 receptors on host cells, primarily in the respiratory tract, initiating infection. Understanding this mechanism is crucial, as it forms the basis for both COVID-19 pathogenesis and vaccine design.
Vaccines like Pfizer-BioNTech and Moderna utilize mRNA technology to instruct our cells to produce a harmless version of the spike protein. This triggers an immune response, generating antibodies and memory cells that recognize and neutralize the actual virus upon exposure. Think of it as a "wanted poster" for the immune system, priming it to identify and attack the real threat.
While the spike protein is essential for viral entry, its presence in vaccines is carefully engineered to be safe and effective. Unlike the virus itself, the vaccine-induced spike protein lacks the genetic material needed for replication, preventing it from causing disease. Furthermore, the mRNA in vaccines degrades quickly after delivering its instructions, leaving no lasting trace in the body.
Dosage plays a critical role in vaccine efficacy. Clinical trials determined optimal doses (30 µg for Pfizer-BioNTech, 100 µg for Moderna) to elicit a robust immune response without excessive side effects. These doses are administered in two shots, spaced 3-4 weeks apart, allowing the immune system to build a strong memory of the spike protein.
For individuals aged 12 and above, these mRNA vaccines have proven highly effective in preventing severe illness, hospitalization, and death from COVID-19. While breakthrough infections can occur, vaccinated individuals typically experience milder symptoms, highlighting the success of spike protein-based vaccines in inducing protective immunity.
Exploring Hawaii's Banking Landscape: Key Financial Institutions in the Islands
You may want to see also
Explore related products






![]()
Vaccine Design: How mRNA and viral vector vaccines encode spike proteins
The COVID-19 pandemic spurred unprecedented innovation in vaccine technology, with mRNA and viral vector vaccines emerging as frontrunners. Both platforms share a common goal: instructing our cells to produce the SARS-CoV-2 spike protein, the key antigen triggering immune protection. However, they achieve this through distinct molecular mechanisms.
MRNA vaccines, exemplified by Pfizer-BioNTech and Moderna, deliver genetic blueprints in the form of messenger RNA encased in lipid nanoparticles. Upon injection, these nanoparticles fuse with muscle cells at the injection site, releasing mRNA molecules. Cellular machinery then reads the mRNA instructions, synthesizing spike proteins. This process mimics natural viral infection without the risk of causing disease. Notably, mRNA is fragile, necessitating ultra-cold storage for stability. Dosing typically involves two 30-microgram injections administered 3-4 weeks apart for individuals aged 12 and above, with lower doses for younger age groups.
Viral vector vaccines, such as AstraZeneca and Johnson & Johnson, employ a different strategy. They utilize harmless adenoviruses, modified to carry the gene encoding the SARS-CoV-2 spike protein. These vectors infect cells, delivering their genetic payload to the nucleus. Unlike mRNA, which remains in the cytoplasm, DNA is transcribed into mRNA, which then directs spike protein synthesis. A single dose of 0.5 mL is standard for adults, with Johnson & Johnson offering a one-shot regimen and AstraZeneca requiring a second dose 4-12 weeks later. This approach leverages established viral delivery systems but carries a rare risk of vaccine-induced immune thrombotic thrombocytopenia (VITT), particularly in younger populations.
Comparing these platforms reveals trade-offs. mRNA vaccines boast higher efficacy rates, often exceeding 90% after two doses, but require stringent cold chain logistics. Viral vector vaccines offer logistical advantages, including refrigerator-stable storage, but demonstrate slightly lower efficacy, around 60-70%. Both induce robust neutralizing antibodies and T-cell responses, crucial for long-term immunity. However, the transient nature of mRNA ensures it degrades quickly, minimizing potential off-target effects, while viral vectors persist longer, raising theoretical concerns about genomic integration, though evidence suggests this risk is negligible.
Practical considerations further differentiate these vaccines. mRNA vaccines’ rapid development and scalability make them ideal for addressing emergent variants through sequence updates. Viral vector vaccines, while slower to adapt, benefit from decades of research in gene therapy, providing a proven safety profile. For individuals with specific concerns, such as needle phobia or pre-existing conditions, understanding these nuances can guide informed decision-making. Ultimately, both technologies represent groundbreaking advancements, offering safe and effective protection against COVID-19 through precise encoding of the spike protein.
mRNA vs. Inactivated Vaccines: Which Offers Superior Protection and Safety?
You may want to see also
Explore related products






![]()
Safety Concerns: Addressing myths about spike protein toxicity or side effects
The spike protein, a key component of COVID-19 vaccines, has been at the center of misinformation campaigns, with claims suggesting it causes toxicity or severe side effects. However, scientific evidence consistently demonstrates that the spike protein in vaccines is safe and does not lead to long-term harm. Unlike the virus itself, the vaccine introduces only a harmless fragment of the spike protein, designed to trigger an immune response without causing illness. This distinction is critical for understanding why vaccines are a protective tool, not a source of danger.
Consider the mechanism: mRNA vaccines, like Pfizer and Moderna, deliver genetic instructions for cells to produce a temporary, non-toxic version of the spike protein. This process occurs in small, controlled amounts—typically just micrograms per dose—far below any threshold that could overwhelm the body. Viral vector vaccines, such as Johnson & Johnson, use a different delivery system but achieve the same goal: presenting the spike protein to the immune system without introducing the virus’s harmful components. Both methods ensure the spike protein is recognized as foreign, prompting antibody production without causing disease.
One persistent myth is that the spike protein damages organs or causes blood clots. Studies, including peer-reviewed research published in *Nature* and *The New England Journal of Medicine*, have found no evidence linking the vaccine-generated spike protein to such effects. In contrast, COVID-19 infection itself poses a far greater risk of blood clots, heart inflammation, and other complications due to the uncontrolled viral replication and systemic inflammation it triggers. Vaccines, by comparison, offer a precise and limited exposure, minimizing risks while maximizing protection.
For those concerned about side effects, it’s important to differentiate between normal immune responses and adverse reactions. Common side effects like fatigue, headache, or soreness are signs the immune system is responding appropriately, not indicators of toxicity. These symptoms typically resolve within days and can be managed with over-the-counter pain relievers, hydration, and rest. Severe reactions are exceedingly rare, occurring in fewer than 5 cases per million doses, and are closely monitored by health authorities worldwide.
Practical steps can further alleviate concerns. First, consult reputable sources like the CDC, WHO, or local health departments for accurate information. Second, discuss individual health conditions with a healthcare provider to address specific concerns. Finally, report any unusual symptoms post-vaccination through official channels, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S., to contribute to ongoing safety monitoring. By grounding decisions in evidence and expert guidance, individuals can confidently separate myth from reality regarding spike protein safety.
Master SBI Bank Exam Preparation: Strategies, Tips, and Study Plan
You may want to see also
Explore related products





![]()
Immune Response: How the body recognizes and responds to the spike protein
The spike protein, a key component of the SARS-CoV-2 virus, has been a focal point in vaccine development. When introduced through vaccines, this protein triggers a precise immune response, teaching the body to recognize and combat the virus without causing illness. This process hinges on the immune system’s ability to identify foreign invaders and mount a defense, a mechanism that has been finely tuned by mRNA and viral vector vaccines.
Recognition Phase: The Immune System’s Surveillance
The immune system’s first step is to detect the spike protein as non-self. Antigen-presenting cells (APCs), such as dendritic cells, engulf the protein and break it into smaller fragments. These fragments are then displayed on the APC’s surface via major histocompatibility complex (MHC) molecules. T cells, the orchestrators of the immune response, scan these fragments. When a T cell’s receptor matches the spike protein fragment, it activates, initiating a cascade of immune reactions. This recognition is critical, as it distinguishes the spike protein from the body’s own proteins, ensuring a targeted response.
Response Phase: Antibody Production and Cellular Defense
Once activated, helper T cells release signaling molecules called cytokines, which recruit B cells. B cells mature into plasma cells, producing antibodies specifically designed to bind to the spike protein. These antibodies neutralize the protein, preventing it from attaching to human cells. Simultaneously, cytotoxic T cells identify and destroy any cells already infected by the virus. This dual response—humoral (antibodies) and cellular (T cells)—creates a robust defense. For instance, mRNA vaccines like Pfizer-BioNTech and Moderna deliver genetic instructions for the spike protein, prompting the body to produce it in small, safe amounts, sufficient to elicit this immune memory.
Practical Considerations: Dosage and Timing
Vaccine efficacy relies on dosage precision and timing. A typical mRNA vaccine regimen involves two doses, 3–4 weeks apart, with a booster dose recommended 6 months later for sustained immunity. For example, the Pfizer vaccine delivers 30 micrograms of mRNA per dose, while Moderna uses 100 micrograms. These doses are calibrated to maximize immune response without overwhelming the system. Age-specific considerations also apply; individuals over 65 or immunocompromised may require additional boosters due to waning immunity.
Comparative Insight: Natural Infection vs. Vaccination
While natural infection exposes the body to the entire virus, vaccines present only the spike protein, minimizing risks like severe illness or long COVID. Studies show that vaccinated individuals produce higher levels of neutralizing antibodies compared to those who recovered from COVID-19. This controlled exposure via vaccines ensures the immune system learns to combat the virus efficiently, reducing hospitalization rates by over 90% in fully vaccinated populations.
Takeaway: The Spike Protein as a Safe Immune Trainer
The spike protein in vaccines acts as a blueprint for immune preparedness. By mimicking the virus’s key component, it trains the body to respond swiftly and effectively without the dangers of actual infection. Understanding this process underscores the importance of vaccination not just for individual protection but also for community immunity. Practical steps, like adhering to recommended dosages and staying updated with boosters, ensure this immune training remains robust against evolving variants.
Understanding Bank Reserves: A Step-by-Step Calculation Guide
You may want to see also
Explore related products






![]()
Variants and Efficacy: Impact of spike protein mutations on vaccine effectiveness
The SARS-CoV-2 spike protein, a key target of COVID-19 vaccines, has undergone numerous mutations in emerging variants, raising concerns about vaccine efficacy. These mutations, particularly in the receptor-binding domain (RBD), can alter the virus's ability to evade immune responses generated by vaccines. For instance, the Omicron variant harbors over 30 spike protein mutations, some of which reduce antibody neutralization by up to 40-fold compared to earlier strains. This underscores the critical need to understand how spike protein mutations impact vaccine effectiveness.
Analyzing the impact of these mutations requires a multi-faceted approach. Laboratory studies using pseudovirus neutralization assays have shown that vaccines like Pfizer-BioNTech and Moderna retain efficacy against many variants, albeit with reduced neutralizing antibody titers. For example, a study in *Nature Medicine* (2022) found that while neutralizing titers against Omicron were lower, a third mRNA vaccine dose restored protection to levels comparable to those against the Delta variant. However, real-world data must complement these findings, as factors like waning immunity and variant prevalence play significant roles in vaccine performance.
From a practical standpoint, booster doses have emerged as a key strategy to counteract the impact of spike protein mutations. The CDC recommends a second booster for individuals over 50 or immunocompromised, as studies show a 70-80% reduction in severe disease after a fourth dose. Additionally, variant-specific vaccines are under development, with clinical trials evaluating Omicron-adapted formulations. These efforts aim to enhance immune recognition of mutated spike proteins, ensuring sustained protection against evolving variants.
Comparatively, the impact of spike protein mutations varies across vaccine platforms. mRNA vaccines, which encode the full-length spike protein, have shown greater adaptability to mutations than adenovirus-vectored vaccines, which may elicit narrower immune responses. For instance, a study in *The Lancet* (2021) reported that AstraZeneca’s vaccine had reduced efficacy against the Beta variant, while mRNA vaccines maintained higher effectiveness. This highlights the importance of platform-specific considerations in vaccine design and deployment.
In conclusion, spike protein mutations in SARS-CoV-2 variants pose a dynamic challenge to vaccine efficacy, but proactive measures can mitigate their impact. Regular monitoring of variant-specific immune responses, strategic booster campaigns, and platform-specific adaptations are essential to maintaining protection. For individuals, staying up-to-date with recommended vaccine doses and following public health guidelines remains the most effective way to combat the evolving virus. As variants continue to emerge, a nuanced understanding of spike protein mutations will be pivotal in guiding vaccine strategies and preserving global health.
Is CJ Banks Closing? Analyzing the Retailer's Business Status
You may want to see also
Frequently asked questions
The spike protein in the COVID-19 vaccines is a harmless, lab-created copy of the one found on the SARS-CoV-2 virus. It teaches the immune system to recognize and fight the virus without causing illness.
No, the spike protein from the vaccine is quickly broken down by the body and does not cause long-term health issues. Extensive research and monitoring confirm the vaccines are safe and effective.
No, the spike protein produced by the vaccine does not shed or transmit to others. It remains in the vaccinated person’s body and is eventually cleared naturally.
No, the spike protein from the vaccine does not affect fertility or pregnancy. Studies show COVID-19 vaccines are safe for pregnant individuals and those planning to conceive.