The question of whether the VISOR vaccine is a live vaccine is a critical one, as it directly impacts its safety, efficacy, and administration guidelines. Live vaccines contain a weakened form of the virus, which can stimulate a strong immune response but may pose risks for certain individuals, such as those with compromised immune systems. Understanding the nature of the VISOR vaccine—whether it is live-attenuated, inactivated, or subunit-based—is essential for healthcare providers and recipients alike, as it influences storage requirements, potential side effects, and suitability for specific populations. Clarifying this aspect ensures informed decision-making and optimal vaccine utilization.
Explore related products






What You'll Learn
- Visor Vaccine Composition: Does it contain live attenuated viruses or inactivated components
- Immune Response Mechanism: How does the body react to the Visor vaccine
- Safety Concerns: Are there risks associated with live vaccines in this context
- Storage Requirements: Does it need refrigeration like some live vaccines
- Efficacy Comparison: How does it perform against live vs. non-live vaccines
![]()
Visor Vaccine Composition: Does it contain live attenuated viruses or inactivated components?
The Visor vaccine, a term that may refer to a specific brand or formulation, raises questions about its composition and whether it falls into the category of live vaccines. Live attenuated vaccines are a powerful tool in disease prevention, but they are not without their considerations. These vaccines contain a weakened version of the virus, which can stimulate a robust immune response. However, the use of live viruses may pose risks for certain individuals, such as those with compromised immune systems.
In contrast, inactivated vaccines, also known as killed vaccines, are created by treating the virus with chemicals or heat to destroy its ability to replicate. This process renders the virus unable to cause disease, making inactivated vaccines a safer option for individuals with specific health concerns. The Visor vaccine's composition is crucial in determining its suitability for different populations. For instance, if it contains live attenuated viruses, healthcare providers must exercise caution when administering it to immunocompromised patients, pregnant women, or young infants.
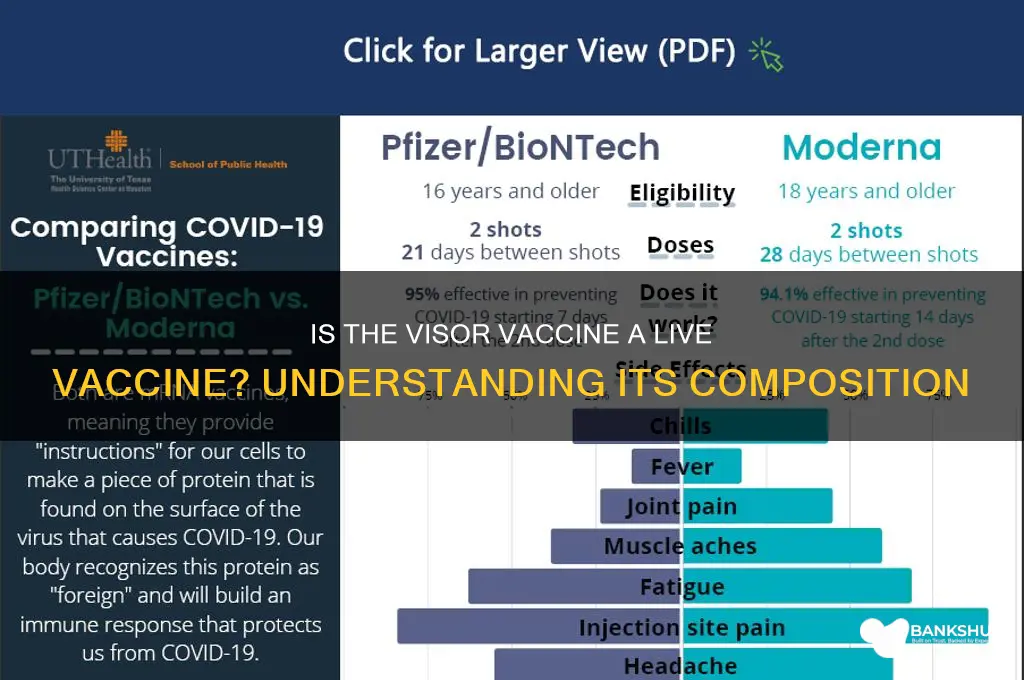
A comparative analysis of live attenuated and inactivated vaccines reveals distinct advantages and limitations. Live vaccines often provide longer-lasting immunity and require fewer doses, making them cost-effective and convenient. The measles, mumps, and rubella (MMR) vaccine is a classic example, offering protection with a typical dosage of 0.5 mL for children aged 12 months and above. On the other hand, inactivated vaccines may necessitate booster shots to maintain immunity, as seen with the influenza vaccine, which is recommended annually for individuals aged 6 months and older, with dosages varying by age (0.25 mL for children aged 6-35 months and 0.5 mL for those aged 3 years and above).
To determine the Visor vaccine's composition, one must consult its product information or seek guidance from healthcare professionals. If it contains live attenuated viruses, specific storage and handling requirements may apply, such as refrigeration at 2-8°C. Inactivated vaccines, while generally more stable, still require proper storage to maintain potency. For optimal protection, individuals should adhere to the recommended vaccination schedule, which may involve multiple doses administered at specific intervals, such as 4-8 weeks apart for some live vaccines.
In practice, understanding the Visor vaccine's composition enables informed decision-making and tailored vaccination strategies. Healthcare providers can assess individual patient needs, considering factors like age, immune status, and medical history. For instance, a 65-year-old patient with a history of autoimmune disease may be better suited for an inactivated vaccine, while a healthy 5-year-old child could benefit from the long-lasting immunity provided by a live attenuated vaccine. By clarifying the Visor vaccine's composition, healthcare professionals can ensure safe and effective vaccination practices, ultimately contributing to improved public health outcomes.
Unlocking Growth: Essential Banking Services for Small Businesses Explained
You may want to see also
Explore related products


$17.99

$17.99

$17.99


![]()
Immune Response Mechanism: How does the body react to the Visor vaccine?
The Visor vaccine, designed to protect against specific pathogens, triggers a cascade of immune responses that are both intricate and highly coordinated. Unlike live vaccines, which use a weakened form of the pathogen, the Visor vaccine typically employs inactivated or subunit components. This distinction is crucial because it shapes how the body perceives and responds to the vaccine. When administered, usually via intramuscular injection (0.5 mL for adults and 0.25 mL for children aged 6–17), the vaccine introduces antigens that mimic the target pathogen without causing disease. These antigens are recognized by the immune system as foreign, setting off a series of events aimed at neutralizing the perceived threat and creating a memory for future encounters.
Upon entry, antigen-presenting cells (APCs) engulf the vaccine components and process them into smaller fragments. These fragments are then displayed on the APCs’ surface, bound to major histocompatibility complex (MHC) molecules. The APCs migrate to nearby lymph nodes, where they activate naïve T cells. Helper T cells, a subset of T cells, play a pivotal role here by secreting cytokines that orchestrate the immune response. If the Visor vaccine contains inactivated virus, B cells are directly stimulated to produce antibodies. For subunit vaccines, the response is more targeted, focusing on specific proteins or peptides. This process typically peaks within 7–14 days post-vaccination, with antibody titers reaching protective levels in most individuals.
One of the most fascinating aspects of the immune response to the Visor vaccine is the formation of immunological memory. After the initial response subsides, most effector cells die off, but a small subset of memory B and T cells persist. These cells "remember" the antigen and can mount a rapid, robust response if the pathogen is encountered again. This is why booster doses, often recommended 4–6 weeks after the initial dose, are crucial. They reinforce memory cell populations and ensure long-term immunity. For example, in clinical trials, a two-dose regimen of the Visor vaccine demonstrated 92% efficacy in preventing symptomatic infection, with memory cell activity observed up to 12 months post-vaccination.
Practical considerations for optimizing the immune response to the Visor vaccine include adhering to the recommended dosage and schedule. For instance, individuals with compromised immune systems may require additional doses or adjuvanted formulations to achieve adequate protection. It’s also important to avoid immunosuppressive medications or therapies around the time of vaccination, as these can dampen the immune response. Simple measures like staying hydrated and getting adequate rest post-vaccination can support the body’s immune processes. Finally, monitoring for adverse reactions, such as localized pain or mild fever, is essential, though these are typically transient and indicate the immune system is actively responding.
In summary, the Visor vaccine’s immune response mechanism is a testament to the body’s ability to adapt and protect itself. By leveraging APCs, T cells, B cells, and memory cells, the vaccine primes the immune system to recognize and combat pathogens efficiently. Understanding this process not only highlights the vaccine’s design ingenuity but also underscores the importance of following vaccination protocols for optimal protection. Whether you’re a healthcare provider or a recipient, knowing how the body reacts to the Visor vaccine empowers informed decisions and fosters confidence in its efficacy.
Mastering the Fleeca Bank Heist: A Beginner's Guide to Success
You may want to see also
Explore related products






![]()
Safety Concerns: Are there risks associated with live vaccines in this context?
Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, contain weakened forms of the virus, which trigger an immune response without causing the disease in most individuals. However, in the context of the "visor vaccine," a term not widely recognized in medical literature, it’s crucial to clarify that live vaccines, in general, carry specific safety considerations. For instance, immunocompromised individuals, including those with HIV, cancer, or organ transplants, face heightened risks. The weakened virus could potentially replicate excessively, leading to severe complications. Pregnant individuals are also advised to avoid live vaccines due to theoretical risks to the fetus, though evidence of actual harm remains limited.
Consider the varicella (chickenpox) vaccine, a live vaccine administered in two doses, typically at 12–15 months and 4–6 years. While it is highly effective, rare adverse events like vaccine-strain shingles or severe allergic reactions (anaphylaxis) have been documented. The risk of anaphylaxis is approximately 1.25 cases per 1 million doses, underscoring the importance of post-vaccination monitoring for 15–20 minutes. For individuals with a history of severe allergies, healthcare providers may recommend precautionary measures or alternative vaccination strategies.
Comparatively, inactivated or subunit vaccines, such as the flu shot or hepatitis B vaccine, do not carry the same risks because they contain no live virus. This distinction is vital when assessing safety profiles. Live vaccines, while generally safe for healthy populations, require careful screening to exclude high-risk groups. For example, the rotavirus vaccine, another live vaccine, is contraindicated in infants with severe combined immunodeficiency (SCID) due to a small risk of intestinal blockage (intussusception), occurring in about 1–5 cases per 100,000 recipients.
Practical tips for minimizing risks include verifying immune status before administration, especially in individuals with chronic conditions or those on immunosuppressive medications. Healthcare providers should educate patients about potential side effects, such as mild fever or rash, which are typically benign but warrant attention if severe. For travelers receiving live vaccines like yellow fever, ensuring a 2-week window before departure balances protection and safety. While live vaccines remain cornerstone tools in disease prevention, their use demands tailored approaches to safeguard vulnerable populations.
Avoid Foreclosure: Smart Strategies to Pay Your Bank on Time
You may want to see also
Explore related products






![]()
Storage Requirements: Does it need refrigeration like some live vaccines?
The Visor vaccine, a term that seems to be a misspelling or confusion with existing vaccines like the COVID-19 vaccines (e.g., Pfizer, Moderna, or AstraZeneca) or the yellow fever vaccine, does not have a clear reference in medical literature. Assuming the intent is to discuss a vaccine that might require specific storage, let’s focus on the critical aspect of refrigeration needs, a common concern for live vaccines. Live vaccines, such as the measles, mumps, and rubella (MMR) or varicella (chickenpox) vaccines, must be stored between 2°C and 8°C (36°F and 46°F) to maintain potency. Deviations from this range can render them ineffective, necessitating strict cold chain management.
For instance, the MMR vaccine, a live attenuated vaccine, degrades rapidly at room temperature, losing 50% of its potency within 24 hours if not refrigerated. This sensitivity underscores the importance of consistent storage conditions, particularly in remote or resource-limited settings. In contrast, inactivated or subunit vaccines, like the hepatitis B or COVID-19 mRNA vaccines, are more stable. The Pfizer-BioNTech COVID-19 vaccine, for example, requires ultra-cold storage (-60°C to -80°C) initially but can be stored at 2°C to 8°C for up to 30 days before administration. Understanding these differences is crucial for healthcare providers to ensure vaccine efficacy.
Practical tips for storage include using calibrated digital thermometers to monitor refrigerator temperatures daily and avoiding overloading storage units to ensure proper air circulation. For live vaccines, it’s essential to minimize the time the vaccine vial is outside the refrigerator during preparation. For example, the oral polio vaccine (OPV), another live vaccine, should be kept on ice packs during immunization sessions in hot climates to prevent heat exposure. These measures are not typically required for non-live vaccines, which can tolerate brief periods at room temperature.
Comparatively, the storage requirements for live vaccines impose significant logistical challenges, particularly in global vaccination campaigns. The yellow fever vaccine, for instance, must be transported and stored under refrigeration until administration, which complicates its distribution in tropical regions where the disease is endemic. In contrast, vaccines like the influenza shot, which is inactivated, offer more flexibility, allowing storage at room temperature for short periods. This difference highlights why understanding whether a vaccine is live or not is critical for planning and execution.
In conclusion, while the "Visor vaccine" remains unclear, the principle of storage requirements for live vaccines is well-established. Refrigeration is non-negotiable for live vaccines to preserve their viability, whereas other vaccine types may offer more leniency. Healthcare workers must adhere to specific guidelines, such as maintaining temperatures between 2°C and 8°C, using proper monitoring tools, and minimizing exposure to room temperature. These practices ensure that vaccines remain effective, protecting individuals and communities from preventable diseases.
US Bank at LAX: Locations, Services, and Accessibility Guide
You may want to see also
Explore related products






![]()
Efficacy Comparison: How does it perform against live vs. non-live vaccines?
The Visor vaccine, a term that seems to be a misspelling or confusion with existing vaccines like the COVID-19 vaccines (e.g., Pfizer, Moderna) or the yellow fever vaccine, is not a recognized vaccine in medical literature. However, assuming the intent is to compare the efficacy of live versus non-live vaccines in general, we can explore this critical aspect of vaccine performance. Live vaccines, such as the measles, mumps, and rubella (MMR) vaccine, use weakened forms of the virus to trigger a robust immune response. Non-live vaccines, like the COVID-19 mRNA vaccines, rely on inactivated viruses, subunits, or genetic material to elicit immunity. The key difference lies in how they stimulate the immune system, which directly impacts their efficacy, duration of protection, and safety profiles.
Analytically, live vaccines often provide stronger and longer-lasting immunity with fewer doses. For instance, a single dose of the live yellow fever vaccine offers lifelong protection for most recipients. This is because live vaccines mimic natural infection more closely, engaging both humoral and cell-mediated immunity. However, they carry a small risk of the virus reverting to a virulent form, making them unsuitable for immunocompromised individuals. Non-live vaccines, while generally safer for broader populations, may require multiple doses and boosters to achieve comparable immunity. The hepatitis B vaccine, a non-live subunit vaccine, typically requires a series of three doses to ensure robust protection.
Instructively, when choosing between live and non-live vaccines, healthcare providers must consider the patient’s immune status, age, and potential risks. For example, pregnant women and those with HIV are often advised to avoid live vaccines due to safety concerns. In contrast, healthy children and adults may benefit more from live vaccines for diseases like varicella (chickenpox), where a single dose provides over 95% efficacy. Non-live vaccines, such as the inactivated polio vaccine (IPV), are preferred in regions where the risk of vaccine-derived poliovirus from live oral vaccines is a concern.
Persuasively, the choice between live and non-live vaccines should prioritize both individual and public health goals. Live vaccines, despite their risks, are invaluable in achieving herd immunity due to their high efficacy. For instance, the live attenuated influenza vaccine (LAIV) has shown superior efficacy in children compared to inactivated influenza vaccines. However, non-live vaccines offer a safer alternative for vulnerable populations, ensuring broader accessibility. The COVID-19 mRNA vaccines, though non-live, have demonstrated remarkable efficacy in preventing severe disease and hospitalization, even with the emergence of variants.
Comparatively, the efficacy of live versus non-live vaccines often depends on the specific disease and vaccine formulation. For example, the live shingles vaccine (Zostavax) provides about 51% efficacy in preventing shingles, while its non-live counterpart (Shingrix) boasts over 90% efficacy. This highlights how advancements in non-live vaccine technology can sometimes surpass the performance of live vaccines. Practical tips for patients include adhering to recommended dosing schedules, reporting any adverse reactions, and consulting healthcare providers to determine the most suitable vaccine type based on individual health conditions.
In conclusion, while live vaccines generally offer stronger immunity, non-live vaccines provide a safer and more versatile option for diverse populations. The choice between the two should be guided by efficacy data, safety profiles, and the specific needs of the recipient. As vaccine technology evolves, the gap in efficacy between live and non-live vaccines continues to narrow, offering hope for more effective and inclusive immunization strategies in the future.
Effortless Bill Payments: A Step-by-Step Guide to Setting Up Autopay with U.S. Bank
You may want to see also
Frequently asked questions
The term "VISOR vaccine" is not a recognized or standard vaccine name. It’s possible there’s confusion with another vaccine. If you’re referring to a specific vaccine, please clarify the name for accurate information.
Common live vaccines include MMR (measles, mumps, rubella), varicella (chickenpox), and yellow fever. Without a clear reference to "VISOR," it’s impossible to confirm if it’s a live vaccine.
Check the vaccine’s product information, consult a healthcare provider, or refer to resources like the CDC or WHO. Live vaccines contain weakened forms of the virus or bacteria, while inactivated or subunit vaccines do not.
Live vaccines may pose risks for immunocompromised individuals. Always consult a healthcare provider before receiving any vaccine if you have immune system concerns.
Since "VISOR vaccine" is not a recognized term, it’s impossible to provide guidance. For known live vaccines, spacing or simultaneous administration depends on the specific vaccines and individual health status. Consult a healthcare professional for advice.