The question of what age a child is considered fully vaccinated is a critical aspect of public health, as it ensures children are protected against preventable diseases. In most countries, vaccination schedules are designed to provide immunity at specific stages of a child’s development, typically starting at birth and continuing through early childhood. By following the recommended immunization timeline, children receive essential vaccines such as those for measles, mumps, rubella, polio, and whooping cough. Generally, by the age of 6, most children have completed their primary series of vaccinations, though booster shots may be required later in childhood or adolescence. Full vaccination status not only safeguards individual health but also contributes to herd immunity, protecting vulnerable populations. Parents and caregivers should consult healthcare providers or local health authorities to ensure their child’s vaccinations are up to date and aligned with national guidelines.
| Characteristics | Values |
|---|---|
| Age for Full Vaccination | By 24 months (2 years) |
| Recommended Vaccines | DTaP, IPV, MMR, Hib, Hepatitis A, Hepatitis B, Varicella, Pneumococcal |
| Total Doses by Age 2 | ~20-25 doses (depending on vaccine schedules and combinations) |
| Booster Shots | Some vaccines require boosters between ages 4-6 (e.g., DTaP, IPV, MMR) |
| Influenza Vaccine | Annual flu shots recommended starting at 6 months of age |
| COVID-19 Vaccine | Recommended for children aged 6 months and older (schedule varies) |
| Catch-Up Vaccination | Available for children who start or fall behind on the schedule |
| Country-Specific Variations | Vaccination schedules may differ slightly by country or region |
| Fully Vaccinated Definition | Completion of all age-appropriate doses as per the recommended schedule |
| Source of Information | CDC, WHO, and local health authorities |
Explore related products






What You'll Learn
- Vaccine Schedule Overview: Standard timelines for childhood vaccinations by age and health authority recommendations
- Common Vaccines: Key vaccines like MMR, DTaP, and polio administered during early childhood
- Booster Shots: Importance and timing of booster doses to maintain immunity in children
- Vaccination Milestones: Ages when children complete primary vaccine series (e.g., 2, 4, 6 years)
- Global Variations: Differences in vaccination completion ages across countries and healthcare systems
![]()
Vaccine Schedule Overview: Standard timelines for childhood vaccinations by age and health authority recommendations
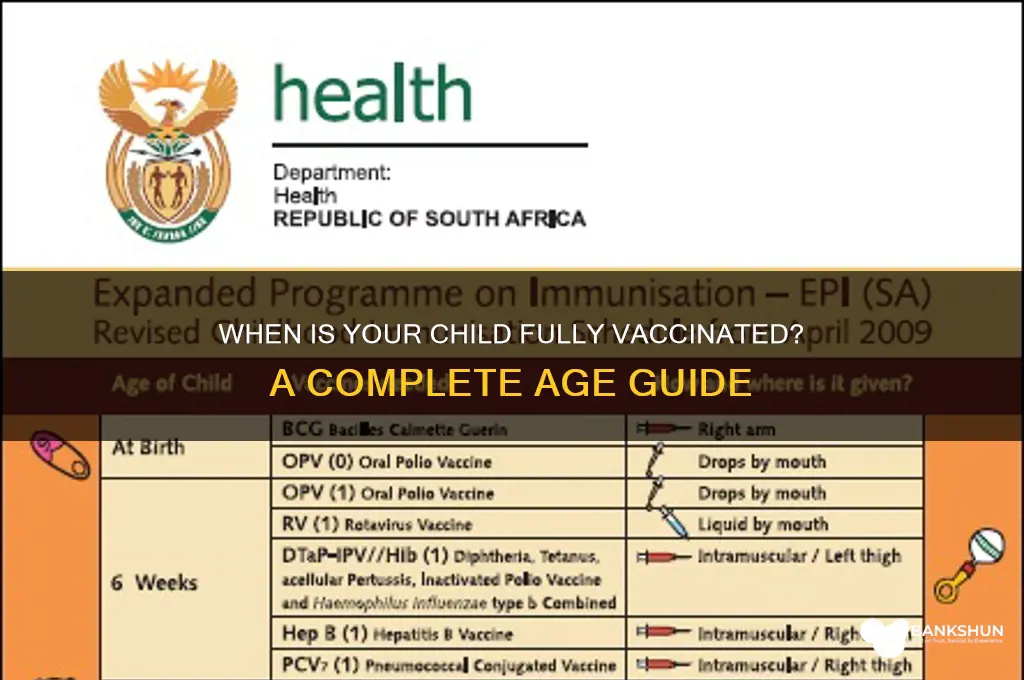
Childhood vaccination schedules are meticulously designed to provide immunity when children are most vulnerable to diseases. The Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) outline timelines that begin at birth, with the first dose of the hepatitis B vaccine typically administered within 24 hours of life. By age 2, a child can receive up to 20 vaccine doses, protecting against diseases like measles, mumps, rubella, polio, and whooping cough. This early start is critical, as infants inherit temporary immunity from their mothers but become susceptible as it wanes. Adhering to this schedule ensures that children are shielded during their most susceptible years, reducing the risk of outbreaks and complications.
The vaccine schedule is not one-size-fits-all; it adapts to age, health status, and regional disease prevalence. For instance, the MMR (measles, mumps, rubella) vaccine is given in two doses, the first at 12–15 months and the second at 4–6 years, aligning with school entry when exposure risk increases. Similarly, the DTaP (diphtheria, tetanus, pertussis) series requires five doses by age 6, with boosters later in childhood. Health authorities like the CDC and WHO emphasize the importance of timely administration, as delays can leave children unprotected during critical developmental stages. Parents should consult healthcare providers to tailor the schedule to their child’s needs, ensuring no dose is missed or inappropriately deferred.
Booster shots play a pivotal role in maintaining immunity as children grow. For example, the Tdap booster, given around age 11–12, reinforces protection against tetanus, diphtheria, and pertussis, while the meningococcal vaccine, administered at 11–12 and 16 years, guards against meningitis. These boosters are not optional—they are essential to sustain immunity that may wane over time. Health authorities also recommend annual flu vaccines starting at six months of age, as influenza strains evolve rapidly. Practical tips include keeping a vaccination record, setting reminders for appointments, and discussing any concerns about side effects with a healthcare provider to ensure informed decision-making.
Global variations in vaccine schedules reflect differences in disease prevalence and healthcare infrastructure. In regions with higher rates of tuberculosis, the BCG vaccine is often given at birth, while in the U.S., it is reserved for high-risk individuals. Similarly, countries with persistent polio transmission may require additional oral polio vaccine doses. These adaptations highlight the importance of local health authority recommendations, which are based on epidemiological data and resource availability. Parents traveling internationally should verify if their child’s vaccinations align with the destination’s requirements, ensuring continuous protection across borders.
By age 18, a child is generally considered fully vaccinated, having completed all recommended doses and boosters. However, "fully vaccinated" is a dynamic term, evolving with new vaccines and disease trends. For instance, the HPV vaccine, now recommended for both boys and girls starting at age 9–12, was not part of earlier schedules. Similarly, COVID-19 vaccines have introduced a new layer of protection for children aged 6 months and older. Staying informed through trusted sources like the CDC, WHO, or local health departments ensures that children receive the most up-to-date protection. Ultimately, adherence to the vaccine schedule is a cornerstone of public health, safeguarding individual children and contributing to community immunity.
Is Pacific Premier Bank Right for You? A Comprehensive Review
You may want to see also
Explore related products






![]()
Common Vaccines: Key vaccines like MMR, DTaP, and polio administered during early childhood
Children typically receive a series of vaccinations during their first six years, with the majority administered by age two. This early schedule is designed to protect them from serious diseases when they are most vulnerable. Among the cornerstone vaccines are MMR (Measles, Mumps, Rubella), DTaP (Diphtheria, Tetanus, Pertussis), and polio, each playing a critical role in childhood immunity.
MMR Vaccine: A Shield Against Three Threats
The MMR vaccine is a combination shot that guards against measles, mumps, and rubella—diseases once common in childhood. The first dose is given between 12 and 15 months, followed by a second dose between ages 4 and 6. This two-dose regimen provides 97% effectiveness against measles and near-complete protection against mumps and rubella. Parents should note that mild fever or rash may occur post-vaccination, but these are normal immune responses and far less severe than the diseases themselves.
DTaP Vaccine: Layered Defense Against Respiratory and Neurological Risks
DTaP protects against diphtheria, tetanus, and pertussis (whooping cough), with doses administered at 2, 4, and 6 months, followed by boosters at 15–18 months and 4–6 years. Pertussis is particularly dangerous for infants, causing violent coughing fits that can lead to pneumonia or brain damage. Tetanus, though rare, can enter the body through minor wounds and cause muscle stiffness or lockjaw. Diphtheria, a respiratory illness, can lead to heart failure. Timely DTaP vaccination not only safeguards the child but also reduces community transmission.
Polio Vaccine: Eradicating a Crippling Disease
Polio vaccination is delivered via the inactivated poliovirus vaccine (IPV), with doses at 2 and 4 months, followed by boosters at 6–18 months and 4–6 years. Polio can cause paralysis or death, but global vaccination efforts have nearly eradicated it. Even in regions where polio is eliminated, vaccination remains critical to prevent reintroduction. Parents should ensure their child completes the full series, as partial immunity leaves them susceptible to this highly contagious virus.
Practical Tips for Parents
To ensure adherence, track vaccine schedules using apps or calendars, and schedule appointments during calm times to minimize stress. For children anxious about needles, distraction techniques like singing or storytelling can help. Keep a record of vaccinations for school enrollment and travel requirements. If a dose is missed, consult a healthcare provider to resume the schedule without restarting.
By following these guidelines for MMR, DTaP, and polio vaccines, parents can provide their children with robust protection against preventable diseases, setting the foundation for lifelong health.
Maximize Your Earnings: Redeeming U.S. Bank Cash Rewards Made Easy
You may want to see also
Explore related products






![]()
Booster Shots: Importance and timing of booster doses to maintain immunity in children
Childhood vaccination schedules are meticulously designed to build robust immunity during critical developmental stages. However, immunity wanes over time, leaving children vulnerable to preventable diseases. Booster shots act as vital reinforcements, replenishing antibody levels and ensuring continued protection. For instance, the diphtheria, tetanus, and pertussis (DTaP) vaccine, administered in a series during infancy, requires a booster dose (DTaP) at 4-6 years of age to maintain immunity through the early school years. This strategic timing bridges the gap between initial vaccination and the need for long-term protection.
Without booster doses, the efficacy of childhood vaccines diminishes, increasing susceptibility to infections like measles, mumps, and whooping cough. These diseases, once common, have been largely controlled through widespread vaccination but remain a threat in under-vaccinated populations. Booster shots not only safeguard individual children but also contribute to herd immunity, protecting those who cannot be vaccinated due to medical reasons. For example, the measles, mumps, and rubella (MMR) vaccine, typically given at 12-15 months and again at 4-6 years, ensures sustained immunity against highly contagious diseases that can cause severe complications.
The timing of booster doses is crucial, as it aligns with the natural decline of vaccine-induced immunity and the evolving immune system of the child. Adolescent boosters, such as the tetanus, diphtheria, and pertussis (Tdap) vaccine recommended at 11-12 years, not only reinforce protection against these diseases but also introduce pertussis immunity to teenagers, a group increasingly affected by whooping cough outbreaks. Similarly, the human papillomavirus (HPV) vaccine, administered in two doses at 11-12 years (or three doses if started after 15), provides long-term protection against cancers caused by HPV infection.
Practical considerations are essential for successful booster administration. Parents should maintain accurate vaccination records and consult healthcare providers to ensure timely scheduling. Schools often require updated immunization records, providing a helpful reminder for booster doses. Additionally, combining booster shots with routine check-ups can streamline the process and minimize missed opportunities. For example, the meningococcal conjugate vaccine (MenACWY), recommended at 11-12 years with a booster at 16, can be administered during adolescent well-visits, ensuring comprehensive protection during a critical period of social and biological development.
In conclusion, booster shots are not optional add-ons but essential components of a child's vaccination journey. They ensure sustained immunity, protect against preventable diseases, and contribute to public health by maintaining herd immunity. By understanding the importance and timing of booster doses, parents and healthcare providers can work together to safeguard children's health throughout their developmental years.
Clostridium Tetani Vaccine: Availability, Effectiveness, and Prevention Explained
You may want to see also
Explore related products






![]()
Vaccination Milestones: Ages when children complete primary vaccine series (e.g., 2, 4, 6 years)
By age 2, most children in the U.S. have completed the primary series of critical vaccines, including MMR (measles, mumps, rubella), varicella (chickenpox), and DTaP (diphtheria, tetanus, pertussis). This milestone marks the first major phase of immunization, protecting against highly contagious diseases that can cause severe complications in early childhood. Parents should ensure their child receives the final doses of these vaccines between 12 and 15 months, followed by a booster for DTaP at 18 months. Missing these doses can leave children vulnerable during their most formative years, so adherence to the CDC’s recommended schedule is essential.
The next vaccination milestone occurs around age 4, when preschoolers receive booster doses to reinforce immunity. Key vaccines at this stage include DTaP, IPV (polio), and MMR, typically administered as a single combination shot. This age is also when children may receive their second dose of the varicella vaccine, ensuring robust protection against chickenpox. Parents should schedule a well-child visit between ages 4 and 6 to confirm all vaccines are up to date before starting kindergarten. Schools often require proof of vaccination, making this a critical checkpoint for compliance and community health.
At age 6, children complete another round of vaccinations, focusing on maintaining immunity through the early school years. The CDC recommends a booster dose of the DTaP vaccine, as well as the first dose of the Tdap vaccine (which includes tetanus, diphtheria, and pertussis) if the DTaP series was completed earlier. Additionally, this age is a good time to administer the annual flu vaccine, which is crucial for preventing seasonal influenza. Parents should also discuss the HPV vaccine with their pediatrician, as the CDC now recommends starting the series at age 9, though some providers begin earlier.
Practical tips for parents include keeping a detailed record of all vaccinations, setting reminders for upcoming doses, and discussing any concerns about side effects with a healthcare provider. While mild reactions like soreness or fever are common, severe adverse events are extremely rare. Staying informed and proactive ensures children reach these vaccination milestones smoothly, safeguarding their health and contributing to herd immunity. Each age-specific series builds upon the last, creating a foundation of protection that lasts a lifetime.
Banks and Mortgages: Who Holds the Power?
You may want to see also
Explore related products






![]()
Global Variations: Differences in vaccination completion ages across countries and healthcare systems
The age at which a child is considered fully vaccinated varies significantly across the globe, influenced by factors such as national health policies, disease prevalence, and healthcare infrastructure. For instance, in the United States, the Centers for Disease Control and Prevention (CDC) recommends that children receive a series of vaccinations from birth to age 6, with key milestones at 2, 4, 6, and 12–15 months. By age 2, a U.S. child typically completes doses for measles, mumps, rubella (MMR), diphtheria, tetanus, pertussis (DTaP), and polio, among others. In contrast, the United Kingdom’s National Health Service (NHS) schedules vaccinations slightly differently, with the MMR vaccine given at 1 year and a booster at 3 years and 4 months, reflecting regional disease risks and public health priorities.
Analyzing these variations reveals how healthcare systems adapt vaccination schedules to local needs. In low-income countries, where vaccine-preventable diseases like measles or polio remain prevalent, immunization often prioritizes early protection. For example, in India, the Universal Immunization Programme administers the first dose of measles vaccine at 9 months, earlier than in high-income nations, due to higher disease transmission rates. Similarly, in sub-Saharan Africa, the World Health Organization (WHO) recommends a birth dose of the hepatitis B vaccine, a practice less common in Europe or North America, to combat higher maternal infection rates. These adjustments highlight the balance between global vaccine standards and localized health challenges.
A comparative look at high-income countries shows how policy choices further diverge. In Japan, the government historically excluded the HPV vaccine from its routine schedule due to public concerns, though it has since been reintroduced. Meanwhile, Australia and Canada include the HPV vaccine for both boys and girls starting at age 9–14, reflecting a proactive approach to cancer prevention. Such differences underscore the role of cultural attitudes, political decisions, and funding in shaping vaccination timelines. For parents navigating these systems, understanding these nuances is crucial, especially when relocating or traveling internationally.
Practical tips for families in a globalized world include verifying vaccination records against destination country requirements and consulting healthcare providers for catch-up schedules if doses are missed. For example, a child moving from a country with a delayed MMR schedule to one with earlier administration may need accelerated dosing to align with local norms. Additionally, travelers should be aware of region-specific vaccines, such as yellow fever in certain African and South American countries, which may not be part of standard childhood schedules elsewhere.
In conclusion, the age of full vaccination for children is not a one-size-fits-all concept but a dynamic framework shaped by regional health needs, policy decisions, and systemic capabilities. By examining these global variations, families and healthcare providers can better navigate the complexities of immunization, ensuring children receive timely protection regardless of where they live or travel.
Unvaccinated Risks: Are Deaths Linked to Missing Vaccines?
You may want to see also
Frequently asked questions
A child is typically considered fully vaccinated by the age of 6, as most routine childhood vaccinations are completed by this age, following the recommended immunization schedule.
No, the definition of "fully vaccinated" can vary depending on factors like geographic location, health guidelines, and individual medical needs. Always consult local health authorities or a pediatrician for specific recommendations.
Some vaccines require booster shots, which are often administered between ages 4 and 6. These boosters ensure continued immunity and are part of being fully vaccinated.
Yes, most children are fully vaccinated by the time they start kindergarten (around age 5-6), as school immunization requirements align with the standard vaccination schedule.
Missing a dose may delay full vaccination status. Consult a healthcare provider to catch up on missed doses and ensure your child is fully protected according to the recommended schedule.