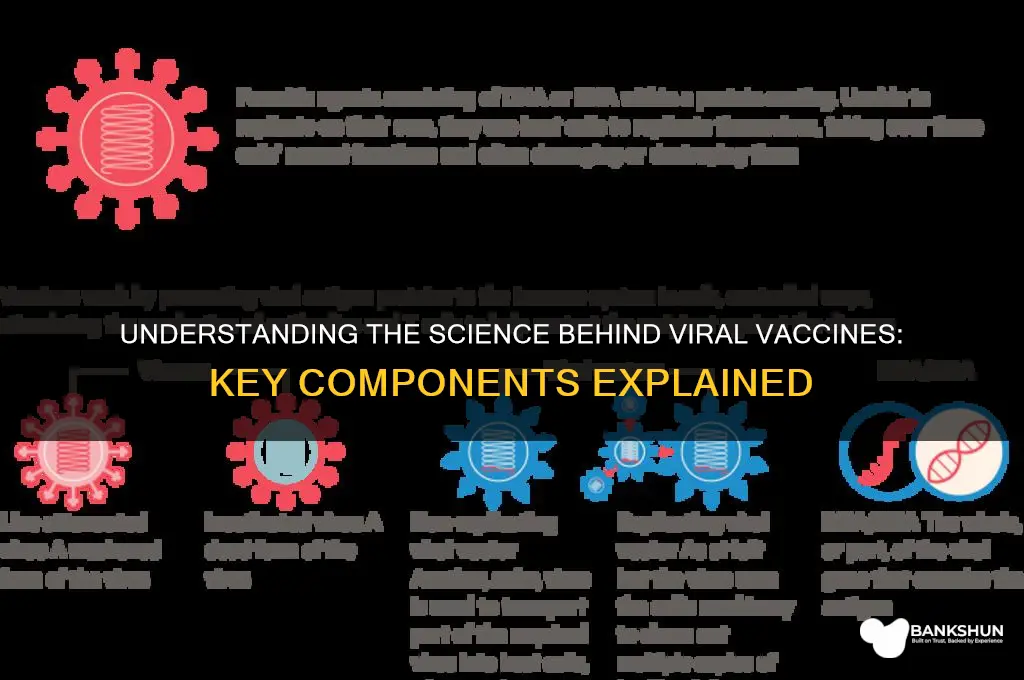
Vaccines against viruses are typically created using a variety of methods that aim to stimulate the immune system to recognize and combat specific viral pathogens. These methods include the use of weakened or inactivated forms of the virus, known as live-attenuated or inactivated vaccines, respectively. Alternatively, vaccines may utilize specific viral components, such as proteins or genetic material, to trigger an immune response without causing the disease. For example, subunit vaccines contain purified pieces of the virus, while mRNA vaccines, like those developed for COVID-19, deliver genetic instructions for cells to produce a harmless viral protein, prompting the immune system to generate protective antibodies and memory cells. Additionally, viral vector vaccines use a different, harmless virus to deliver genetic material from the target virus into cells. Each approach is carefully designed to provide effective protection while ensuring safety and minimizing side effects.
Explore related products






What You'll Learn
- Weakened Viruses: Live attenuated viruses, weakened in labs, trigger immune response without causing disease
- Killed Viruses: Inactivated viruses, destroyed but intact, used to stimulate immune system safely
- Subunit Vaccines: Specific viral proteins or pieces, not whole virus, induce targeted immune response
- mRNA Vaccines: Genetic material encoding viral proteins, prompting cells to produce immune triggers
- Viral Vector Vaccines: Harmless viruses deliver genetic material from target virus to cells
![]()
Weakened Viruses: Live attenuated viruses, weakened in labs, trigger immune response without causing disease
Live attenuated vaccines harness the power of weakened viruses to train the immune system without causing disease. These vaccines contain a version of the virus that has been modified in the lab to reduce its virulence, or ability to cause illness. This attenuation can be achieved through various methods, such as serial passage in cell cultures or targeted genetic modifications. The result is a virus that retains its ability to enter cells and replicate, but at a much lower rate, triggering a robust immune response without the risk of severe infection.
Consider the measles, mumps, and rubella (MMR) vaccine, a classic example of a live attenuated vaccine. The viruses in this vaccine are weakened through repeated cultivation in animal cells, a process that introduces mutations reducing their pathogenicity. When administered as a single subcutaneous dose, typically around 0.5 mL, the vaccine prompts the body to produce antibodies and memory cells specific to these viruses. This immunity is long-lasting, often conferring lifelong protection after a two-dose series, with the first dose given at 12–15 months of age and the second at 4–6 years.
One of the key advantages of live attenuated vaccines is their ability to mimic natural infection, stimulating both humoral (antibody-mediated) and cell-mediated immunity. This dual response is particularly effective against viruses that infect mucosal surfaces, such as influenza or rotavirus. For instance, the nasal spray flu vaccine (LAIV) delivers attenuated influenza viruses directly to the nasal mucosa, where they induce local immune responses that can prevent viral entry. However, this vaccine is not recommended for individuals with weakened immune systems, pregnant women, or children under 2 years old, as the live viruses, though weakened, could pose a risk in these populations.
Despite their efficacy, live attenuated vaccines require careful handling and storage. They are typically stored at 2–8°C (36–46°F) to maintain viral viability, and exposure to heat or light can degrade their potency. Additionally, because these vaccines contain live viruses, they should not be given to individuals with severe immunodeficiency or those undergoing immunosuppressive therapy. For example, the varicella (chickenpox) vaccine, another live attenuated product, is contraindicated in people with HIV/AIDS or cancer, as the weakened virus could potentially cause severe complications in these immunocompromised individuals.
In summary, live attenuated vaccines represent a sophisticated approach to viral immunization, leveraging weakened viruses to safely elicit strong, durable immune responses. Their ability to replicate natural infection makes them highly effective, but their live nature necessitates careful consideration of dosage, administration, and patient suitability. By understanding these nuances, healthcare providers can maximize the benefits of these vaccines while minimizing risks, ensuring broad protection against debilitating viral diseases.
MUFG's Unique Banking Approach: What Sets It Apart from Competitors
You may want to see also
Explore related products






![]()
Killed Viruses: Inactivated viruses, destroyed but intact, used to stimulate immune system safely
Viruses, though microscopic, can wreak havoc on the human body. To combat them, scientists have developed vaccines using various strategies, one of which involves killed viruses. These inactivated viruses, while destroyed, retain their structural integrity, allowing them to safely stimulate the immune system without causing disease. This approach has been successfully employed in vaccines such as the injectable influenza vaccine and the Salk polio vaccine. By presenting the immune system with a harmless version of the virus, these vaccines prompt the production of antibodies and immune memory, preparing the body to fight off future infections.
Consider the process of creating killed virus vaccines: viruses are grown in cell cultures or embryonated eggs, then exposed to chemicals like formaldehyde or heat to inactivate them. This destruction ensures the virus can no longer replicate, eliminating the risk of infection. However, the viral proteins, particularly those on the surface, remain intact, enabling the immune system to recognize and respond to them. For instance, the inactivated polio vaccine contains the three poliovirus serotypes, each treated to preserve their antigenic structure. This method has proven effective in preventing poliomyelitis, particularly in regions where the oral vaccine’s live attenuated viruses pose a risk of vaccine-derived poliovirus outbreaks.
One of the key advantages of killed virus vaccines is their safety profile, especially for individuals with compromised immune systems or specific age groups. For example, the inactivated influenza vaccine is recommended for pregnant women, elderly individuals, and those with chronic conditions, as it eliminates the risk of viral replication associated with live vaccines. Dosage typically involves a single 0.5 mL injection for adults and children over 3 years, with a reduced dose for younger children. However, a notable drawback is that killed vaccines often require multiple doses and adjuvants to enhance immune response, as they may not induce the same level of cellular immunity as live vaccines.
Practical considerations for administering killed virus vaccines include proper storage and handling to maintain vaccine efficacy. Most inactivated vaccines are stored between 2°C and 8°C, with strict adherence to the cold chain to prevent degradation. Healthcare providers should also be aware of potential side effects, such as soreness at the injection site, mild fever, or fatigue, which are generally short-lived. For optimal protection, following the recommended vaccination schedule is crucial, as delays can reduce immunity. For example, the inactivated polio vaccine is typically administered in a series of 3-4 doses starting at 2 months of age, with a booster later in childhood.
In comparison to live attenuated vaccines, killed virus vaccines offer a safer alternative but may require additional measures to achieve robust immunity. While live vaccines mimic natural infection more closely, inactivated vaccines rely on the precise presentation of viral antigens to trigger an immune response. This distinction highlights the importance of tailoring vaccine design to the specific virus and target population. For instance, the killed rabies vaccine, though effective, requires a more complex regimen, including multiple doses and, in some cases, immunoglobulin administration, to ensure protection against this deadly virus. Despite these challenges, killed virus vaccines remain a cornerstone of preventive medicine, providing a safe and reliable means to combat viral diseases.
Understanding FCCR: What It Means and Its Role in Banking
You may want to see also
Explore related products






![]()
Subunit Vaccines: Specific viral proteins or pieces, not whole virus, induce targeted immune response
Subunit vaccines represent a precision tool in the fight against viral infections, harnessing the power of specific viral components rather than the entire pathogen. Unlike traditional vaccines that use weakened or inactivated viruses, subunit vaccines contain only the essential fragments—typically proteins or peptides—that trigger a robust immune response. This approach minimizes the risk of adverse reactions while maximizing efficacy, making it particularly suitable for vulnerable populations such as the elderly, immunocompromised individuals, or young children. For instance, the hepatitis B vaccine, one of the earliest subunit vaccines, uses a single viral protein (hepatitis B surface antigen) to confer long-lasting immunity with minimal side effects.
The development of subunit vaccines involves meticulous identification and isolation of the most immunogenic viral components. These components are often surface proteins that the virus uses to attach to host cells, such as the spike protein in SARS-CoV-2. Once identified, these proteins can be produced through recombinant DNA technology, ensuring purity and consistency. This method allows for large-scale manufacturing without the need to handle live viruses, reducing production risks and costs. For example, the Novavax COVID-19 vaccine uses nanoparticle technology to display the SARS-CoV-2 spike protein, inducing a targeted immune response with a typical two-dose regimen spaced 3–4 weeks apart.
One of the key advantages of subunit vaccines is their safety profile. Because they do not contain live or even inactivated virus, the risk of vaccine-induced illness is virtually eliminated. This makes them ideal for individuals with weakened immune systems or those at risk of severe complications from viral infections. However, their highly specific nature sometimes requires the inclusion of adjuvants—substances that enhance the immune response—to ensure sufficient immunity. Common adjuvants like aluminum salts or lipid nanoparticles are carefully dosed to balance efficacy and safety, with clinical trials often focusing on age-specific formulations. For instance, pediatric subunit vaccines may use lower antigen doses paired with milder adjuvants to suit developing immune systems.
Despite their benefits, subunit vaccines are not without challenges. Their targeted approach can sometimes result in weaker or shorter-lived immunity compared to whole-virus vaccines, necessitating booster doses. Additionally, identifying the right viral components requires extensive research, particularly for rapidly mutating viruses like influenza or HIV. However, advancements in bioinformatics and structural biology are accelerating this process, enabling the design of next-generation subunit vaccines. Practical tips for recipients include adhering to the recommended dosing schedule, monitoring for mild side effects like soreness at the injection site, and consulting healthcare providers for personalized advice, especially for those with pre-existing conditions.
In summary, subunit vaccines exemplify the intersection of precision medicine and immunology, offering a safe and effective strategy to combat viral diseases. By focusing on specific viral proteins, they induce a targeted immune response while minimizing risks, making them a cornerstone of modern vaccination efforts. As technology evolves, their role in addressing both existing and emerging viral threats will only grow, underscoring their importance in global health initiatives.
Brian Banks' NFL Journey: From Exoneration to the Gridiron
You may want to see also
Explore related products






![]()
mRNA Vaccines: Genetic material encoding viral proteins, prompting cells to produce immune triggers
MRNA vaccines represent a groundbreaking shift in how we combat viral infections, leveraging the body’s own cellular machinery to mount a defense. Unlike traditional vaccines that introduce a weakened or inactivated virus, mRNA vaccines deliver genetic instructions—specifically, messenger RNA (mRNA)—that teach cells to produce a harmless piece of the virus, such as the spike protein of SARS-CoV-2. This triggers an immune response, preparing the body to recognize and fight the actual virus if exposed. The elegance of this approach lies in its precision: it targets only the necessary viral component without introducing the virus itself.
Consider the COVID-19 mRNA vaccines, such as Pfizer-BioNTech and Moderna, which have been administered to billions of people worldwide. These vaccines contain lipid nanoparticles encapsulating mRNA strands that encode for the SARS-CoV-2 spike protein. Once injected into the muscle, typically in a 0.3 mL dose for adults and a lower volume for children aged 5–11, the mRNA enters cells and directs protein synthesis. The immune system identifies the foreign protein, produces antibodies, and generates memory cells for future protection. This process mimics natural infection but without the risk of severe disease.
One of the most compelling advantages of mRNA vaccines is their adaptability. Because they rely on genetic material rather than viral components, they can be rapidly redesigned to target new variants or entirely different pathogens. For instance, the COVID-19 mRNA vaccines were updated within months to address the Omicron variant, showcasing their flexibility. This speed is particularly crucial in a pandemic, where viral evolution outpaces traditional vaccine development timelines. However, this innovation requires careful storage—mRNA vaccines must be kept at ultra-cold temperatures (e.g., -70°C for Pfizer) until shortly before administration, which poses logistical challenges in resource-limited settings.
Despite their success, mRNA vaccines are not without limitations. They are less effective in individuals with compromised immune systems, such as those undergoing chemotherapy or living with HIV, as these conditions hinder robust immune responses. Additionally, rare side effects like myocarditis, primarily in young males after the second dose, have been reported, though the risk remains significantly lower than that of severe COVID-19. To mitigate this, health authorities recommend spacing doses by 8 weeks for adolescents and young adults, balancing protection with safety.
In practice, mRNA vaccines exemplify the fusion of biology and technology, offering a template for future vaccine development. Their ability to confer immunity without live viral components makes them safer for immunocompromised populations and eliminates the risk of infection from the vaccine itself. As research advances, mRNA platforms could revolutionize responses to other viruses, such as influenza or HIV, by tailoring vaccines to specific strains or mutations. For now, they stand as a testament to human ingenuity, transforming genetic code into a shield against viral threats.
Correcting Your Name at the Bank: A Step-by-Step Guide to Updating Your Account Information
You may want to see also
Explore related products






![]()
Viral Vector Vaccines: Harmless viruses deliver genetic material from target virus to cells
Viruses, by their nature, hijack cellular machinery to replicate. Viral vector vaccines exploit this very mechanism, but with a clever twist: they use a harmless virus as a Trojan horse to deliver genetic instructions from a target virus into our cells. This triggers an immune response without causing disease, preparing the body to fight the real pathogen if encountered.
Imagine a mail carrier delivering a blueprint instead of a harmful package. The blueprint, in this case, is a gene encoding a specific protein from the target virus, like the spike protein of SARS-CoV-2.
The process is remarkably precise. A weakened or modified virus, often an adenovirus (common cold culprit) or a poxvirus, is engineered to carry the target virus's genetic material. This vector virus is then injected into the body. It enters cells, releasing its cargo – the genetic instructions. The cell's machinery reads these instructions and produces the target virus protein. The immune system recognizes this foreign protein as an intruder, mounting a defense by producing antibodies and activating T-cells. This immune memory equips the body to swiftly recognize and neutralize the actual virus if exposed in the future.
Notably, the vector virus itself is rendered harmless, unable to replicate or cause illness. This safety feature makes viral vector vaccines suitable for a wide range of individuals, including those with compromised immune systems.
The Johnson & Johnson COVID-19 vaccine exemplifies this technology. A single dose of this adenovirus-based vaccine delivers the genetic code for the SARS-CoV-2 spike protein, prompting a robust immune response. Similarly, the AstraZeneca vaccine utilizes a modified chimpanzee adenovirus as its vector. These vaccines offer the advantage of requiring only one dose and being stable at standard refrigerator temperatures, facilitating distribution in diverse settings.
While highly effective, viral vector vaccines can, in rare cases, trigger an unusual blood clotting disorder with low platelets, particularly in younger women. This highlights the importance of informed consent and individualized risk assessment. Overall, viral vector vaccines represent a powerful tool in our fight against infectious diseases, leveraging the very mechanisms viruses use to their advantage, but redirecting them to protect rather than harm. Their adaptability and relative ease of production make them a promising platform for future vaccine development against emerging pathogens.
Understanding Bank CDs: What Does a Certificate of Deposit Mean?
You may want to see also
Frequently asked questions
Vaccines against viruses are typically created from weakened or inactivated viruses, viral proteins, genetic material (like mRNA or DNA), or viral vectors.
Weakened (attenuated) viruses are modified to reduce their virulence but retain their ability to trigger an immune response, while inactivated viruses are completely killed and cannot replicate but still stimulate immunity.
mRNA vaccines, like those for COVID-19, contain genetic instructions that teach cells to produce a harmless viral protein, prompting the immune system to recognize and fight the actual virus.
Viral vectors are harmless viruses modified to deliver genetic material from the target virus into cells, triggering an immune response without causing disease.
Protein-based vaccines use purified pieces of the virus, such as its spike protein, to stimulate the immune system to produce antibodies and immune cells that protect against infection.