The Centers for Disease Control and Prevention (CDC) provide specific recommendations for the meningococcal vaccine to protect individuals from meningococcal disease, a serious bacterial infection that can lead to meningitis and bloodstream infections. The CDC advises routine vaccination for adolescents at 11 or 12 years old, with a booster dose at 16 years old, using the meningococcal conjugate vaccine (MenACWY). Additionally, the CDC recommends the serogroup B meningococcal (MenB) vaccine for certain high-risk groups, such as individuals with complement deficiencies or asplenia, and those exposed to outbreaks. Vaccination is also suggested for college freshmen living in dormitories, military recruits, and travelers to regions with high disease prevalence. These guidelines aim to reduce the incidence of meningococcal disease and its potentially severe complications.
Explore related products






What You'll Learn
- CDC recommends routine meningococcal vaccination for adolescents at age 11-12 years
- A booster dose is advised at age 16 for continued protection
- High-risk groups, including travelers, should receive the vaccine earlier
- Serogroup B vaccine is recommended for specific at-risk populations
- CDC advises vaccination for teens and young adults through age 23
![]()
CDC recommends routine meningococcal vaccination for adolescents at age 11-12 years
The CDC's recommendation for routine meningococcal vaccination at age 11-12 years is a critical preventive measure against a potentially life-threatening bacterial infection. Meningococcal disease, caused by *Neisseria meningitidis*, can lead to meningitis (inflammation of the brain and spinal cord) and septicemia (blood infection), with rapid onset and high fatality rates. Adolescents are at increased risk due to behaviors like sharing utensils or living in close quarters, which facilitate bacterial transmission. The CDC advises a single dose of the meningococcal conjugate vaccine (MenACWY) during this age range to build immunity before peak risk years (16-21 years).
From a practical standpoint, parents and caregivers should schedule the MenACWY vaccine alongside the Tdap booster and HPV vaccine series, typically administered during the preteen checkup. This bundling approach ensures comprehensive protection during a single visit, minimizing disruptions to school or extracurricular activities. The vaccine is safe, with common side effects limited to mild pain, redness at the injection site, or low-grade fever. It’s important to note that this initial dose is followed by a booster at age 16 to maintain immunity through young adulthood, a period of heightened vulnerability.
A comparative analysis highlights the vaccine’s effectiveness: MenACWY covers four serogroups (A, C, W, Y) responsible for 70% of U.S. meningococcal cases. While a separate vaccine (MenB) exists for serogroup B, the CDC does not recommend it routinely for all adolescents, reserving it for specific high-risk groups or during outbreaks. This distinction underscores the tailored nature of the CDC’s guidance, balancing public health impact with individual risk profiles. For adolescents with conditions like asplenia or complement deficiencies, additional doses or earlier vaccination may be warranted—a reminder to consult healthcare providers for personalized advice.
Persuasively, the case for timely vaccination rests on the disease’s severity and the vaccine’s proven track record. Meningococcal disease progresses rapidly, often within hours, leaving little time for treatment. Even with antibiotics, 10-15% of infected individuals die, and 10-20% of survivors suffer long-term disabilities such as limb loss, hearing impairment, or neurological damage. Vaccination not only protects the individual but also reduces bacterial circulation in communities, a concept known as herd immunity. By adhering to the CDC’s 11-12-year recommendation, families contribute to broader disease prevention while safeguarding their child’s health.
In conclusion, the CDC’s routine meningococcal vaccination recommendation for 11-12-year-olds is a proactive, evidence-based strategy to combat a rare but devastating disease. By integrating this vaccine into preteen healthcare routines, parents and providers can ensure adolescents are shielded during their highest-risk years. Practical steps, such as combining vaccinations and staying informed about booster schedules, maximize protection with minimal effort. This approach exemplifies preventive medicine at its best—simple, effective, and potentially life-saving.
Mastering SC2 Bank Mods: Enhance Your Crap Patrol Experience
You may want to see also
Explore related products






![]()
A booster dose is advised at age 16 for continued protection
The CDC's recommendation for a meningococcal vaccine booster at age 16 is rooted in the waning immunity observed after the initial vaccination, typically administered during adolescence. Studies indicate that protective antibody levels can decrease significantly within 5 years of the first dose, leaving individuals vulnerable to meningococcal disease during late adolescence and early adulthood—a period marked by increased risk due to lifestyle factors like crowded living conditions (e.g., college dormitories) and behavioral patterns. This booster dose, ideally given as MenACWY, reinforces immunity against serogroups A, C, W, and Y, which are responsible for the majority of cases in the United States.
From a practical standpoint, scheduling this booster dose at age 16 aligns with routine healthcare visits, such as the annual check-up or sports physical, minimizing the need for an additional appointment. Parents and caregivers should ensure that the vaccine is administered as a single 0.5 mL intramuscular injection, preferably in the deltoid muscle. It’s crucial to verify the patient’s vaccination history, as those who received their first dose before age 10 require two doses for adequate protection, with the booster given at least 8 weeks after the second dose. Adhering to this schedule maximizes the vaccine’s efficacy and ensures prolonged immunity during critical years.
A comparative analysis highlights the importance of this booster in contrast to other adolescent vaccines. While vaccines like Tdap and HPV also target this age group, the meningococcal booster stands out due to the rapid decline in antibody titers post-initial vaccination. For instance, Tdap immunity wanes more gradually, and HPV vaccination relies on a series completed before potential exposure. The meningococcal booster, however, addresses a more immediate vulnerability, particularly as teens transition to higher-risk environments like college campuses, where outbreaks are more likely to occur.
Persuasively, the case for this booster dose is strengthened by its role in preventing severe, life-threatening complications of meningococcal disease, such as meningitis and sepsis. These conditions progress rapidly, often within hours, and can lead to long-term disabilities or death even with prompt treatment. By maintaining robust immunity through the booster, individuals not only protect themselves but also contribute to herd immunity, reducing the disease’s spread in communities. This dual benefit underscores the booster’s significance as a public health measure, not just an individual safeguard.
Finally, a descriptive approach illustrates the real-world impact of adhering to this recommendation. Imagine a college freshman who received their meningococcal booster at age 16, as advised. When an outbreak occurs in their dorm, they remain asymptomatic while unvaccinated peers fall ill. This scenario underscores the booster’s role in providing uninterrupted protection during a high-risk phase of life. Practical tips for ensuring compliance include setting calendar reminders, discussing the booster with school nurses, and leveraging electronic health records to track vaccination status. Such proactive measures transform a simple recommendation into a lifesaving practice.
Step-by-Step Guide to Removing Your Banks Ram Air Filter
You may want to see also
Explore related products






![]()
High-risk groups, including travelers, should receive the vaccine earlier
The CDC emphasizes that certain high-risk groups, including travelers to regions with endemic meningococcal disease, should prioritize early vaccination. This recommendation stems from the heightened vulnerability of these individuals to infection, particularly in areas where the disease is more prevalent. For instance, the "meningitis belt" in sub-Saharan Africa experiences seasonal outbreaks, making vaccination a critical preventive measure for travelers. The CDC advises that such individuals receive the meningococcal vaccine at least 1–2 weeks before departure to ensure adequate immune response. This proactive approach not only protects the traveler but also helps prevent the spread of the disease across borders.
Analyzing the specifics, the CDC recommends the MenACWY vaccine for travelers to high-risk areas, with a single dose sufficient for most adults. For adolescents aged 11–18, a booster dose is advised after 5 years, while adults in high-risk categories may require additional doses based on ongoing exposure. Notably, the MenB vaccine, which protects against a different serogroup, is not routinely recommended for travelers unless they have specific risk factors, such as complement deficiencies or spleen removal. This tailored approach ensures that vaccination efforts are both effective and resource-efficient.
From a practical standpoint, travelers should consult healthcare providers 4–6 weeks before their trip to discuss vaccination needs. This timeline allows for vaccine administration and immune system response, as well as addressing any potential side effects, which are generally mild (e.g., soreness at the injection site, headache). Travelers should also be aware of local health advisories and carry proof of vaccination, as some countries may require it for entry during outbreak periods. Combining vaccination with other preventive measures, such as avoiding close contact with sick individuals, further reduces risk.
Persuasively, early vaccination for high-risk groups is not just a health recommendation—it’s a responsibility. Meningococcal disease progresses rapidly, with symptoms like fever, headache, and stiff neck escalating to life-threatening complications within hours. For travelers, the stakes are even higher, as access to medical care in remote or resource-limited areas may be delayed. By prioritizing vaccination, individuals protect not only themselves but also vulnerable populations in their destinations. This dual benefit underscores the importance of adhering to CDC guidelines, ensuring safer travel and global health security.
Comparatively, while routine childhood immunization schedules include meningococcal vaccines, high-risk groups often require accelerated or additional dosing. For example, college students living in dormitories and military personnel in barracks are also considered high-risk due to close living conditions, but their vaccination timelines differ from those of travelers. Travelers, however, face the added challenge of exposure to unfamiliar strains in new environments, making early vaccination particularly critical. This distinction highlights the need for personalized vaccination strategies based on individual risk profiles, a principle central to the CDC’s recommendations.
Bank Teller: Who Are They and What Do They Do?
You may want to see also
Explore related products






![]()
Serogroup B vaccine is recommended for specific at-risk populations
The CDC's recommendations for the meningococcal serogroup B vaccine are tailored to protect those most vulnerable to this rare but severe disease. Unlike the meningococcal conjugate vaccine (MenACWY), which targets serogroups A, C, W, and Y, the serogroup B vaccine (MenB) is not routinely recommended for all adolescents. Instead, it is strategically advised for specific at-risk populations, ensuring targeted prevention where the threat is highest.
Identifying At-Risk Groups:
The CDC identifies several populations at heightened risk for serogroup B meningococcal disease. These include individuals aged 10 years or older with persistent complement component deficiencies (e.g., C5–C9, properdin, factor H, or factor D), those without a spleen or with spleen dysfunction, and people exposed during a serogroup B outbreak. Microbiologists routinely exposed to *Neisseria meningitidis* isolates in laboratory settings are also considered at-risk. For these groups, the MenB vaccine is not optional—it’s a critical preventive measure.
Vaccination Schedule and Dosage:
The MenB vaccine is administered in a series of doses, with the exact schedule depending on the vaccine brand. Bexsero® requires two doses for individuals aged 10–25 years, spaced at least one month apart, while Trumenba® typically involves three doses: the first two given one to two months apart, followed by a third dose six months after the first. For those at highest risk, such as those with complement deficiencies or asplenia, adhering to this schedule is essential to ensure optimal protection.
Practical Considerations for Implementation:
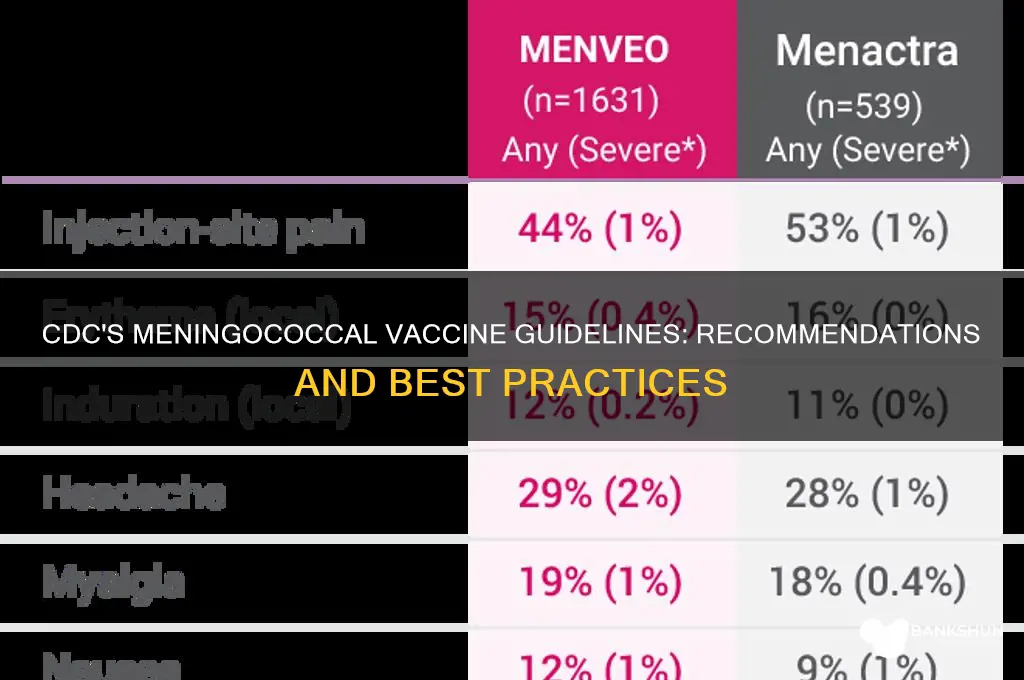
Healthcare providers must carefully assess patient history to determine eligibility for the MenB vaccine. For example, individuals with a history of Guillain-Barré syndrome should be evaluated on a case-by-case basis, as the vaccine may pose risks. Additionally, providers should educate patients about potential side effects, such as pain at the injection site, fatigue, and headache, which are generally mild and short-lived. Clear communication ensures informed decision-making and fosters trust in the vaccination process.
Comparative Perspective:
While MenACWY is recommended for all preteens and teens, the MenB vaccine’s targeted approach reflects its narrower scope of protection. This distinction highlights the importance of precision in public health strategies. By focusing on at-risk populations, the CDC maximizes the vaccine’s impact while minimizing unnecessary interventions for the general population. This tailored approach serves as a model for how vaccines can be deployed effectively in diverse communities.
Takeaway for Public Health:
The CDC’s recommendation for the MenB vaccine underscores the principle of risk-based prevention. By identifying and protecting specific at-risk groups, public health officials can reduce the burden of serogroup B meningococcal disease without overburdening the healthcare system. For clinicians, pharmacists, and patients, understanding these guidelines is crucial for implementing timely and appropriate vaccination strategies. In the fight against meningococcal disease, precision is as vital as prevention.
Deutsche Bank's Leadership Structure: Managing Directors Count Explained
You may want to see also
Explore related products


![]()
CDC advises vaccination for teens and young adults through age 23
The CDC's recommendation for meningococcal vaccination among teens and young adults through age 23 is rooted in the heightened vulnerability of this age group to meningococcal disease. Adolescents and young adults are at increased risk due to factors like living in close quarters (e.g., college dormitories) and behaviors that facilitate bacterial transmission, such as sharing drinks or kissing. Meningococcal disease, caused by *Neisseria meningitidis*, can lead to severe complications like meningitis and septicemia, progressing rapidly and becoming life-threatening within hours. Vaccination is a critical preventive measure, offering protection against the most common serogroups (A, C, W, and Y) responsible for disease in the U.S.
The CDC advises that all preteens receive the first dose of the meningococcal conjugate vaccine (MenACWY) at age 11 or 12, followed by a booster dose at age 16 to maintain immunity during the years of highest risk. For teens who missed the initial vaccination, the CDC recommends starting the series as soon as possible, ensuring they receive the booster dose by age 18. Young adults aged 18–23, particularly those living in college dormitories or military barracks, are also encouraged to receive a dose of MenACWY if they did not receive it at age 16. Additionally, the CDC recommends the serogroup B meningococcal (MenB) vaccine for individuals aged 16–23, preferably between ages 16 and 18, though the decision should be made in consultation with a healthcare provider.
Practical considerations for vaccination include scheduling doses during routine healthcare visits, such as annual check-ups or back-to-school appointments. Parents and young adults should be aware that the MenACWY and MenB vaccines are separate, and both may be necessary for comprehensive protection. Side effects are generally mild, including soreness at the injection site, headache, or fatigue, and typically resolve within a few days. Cost should not be a barrier, as most insurance plans cover meningococcal vaccines, and programs like the Vaccines for Children (VFC) program provide free vaccines for eligible children.
Comparatively, the CDC’s focus on teens and young adults contrasts with recommendations for other age groups, where vaccination is less frequently advised unless specific risk factors are present. This targeted approach reflects the epidemiological data showing that 70% of meningococcal disease cases in the U.S. occur in adolescents and young adults. By prioritizing this demographic, the CDC aims to reduce disease incidence and prevent outbreaks in high-risk settings. For example, college freshmen living in dormitories are 3.5 times more likely to contract meningococcal disease than their peers living off-campus, underscoring the importance of timely vaccination.
In conclusion, the CDC’s recommendation for meningococcal vaccination among teens and young adults through age 23 is a proactive strategy to protect a high-risk population from a potentially deadly disease. By adhering to the advised vaccination schedule—MenACWY at ages 11–12 and 16, and MenB for those aged 16–23—individuals can significantly reduce their risk of infection. Parents, healthcare providers, and young adults themselves play a crucial role in ensuring compliance, as timely vaccination not only safeguards individual health but also contributes to community-wide protection against meningococcal disease.
How Banks Are Innovating to Win Over Millennial Customers
You may want to see also
Frequently asked questions
The CDC recommends that all preteens and teens receive the meningococcal conjugate vaccine (MenACWY) at age 11 or 12, followed by a booster dose at age 16.
No, the CDC does not routinely recommend MenB for everyone. It is recommended for individuals aged 10 years or older who are at increased risk, such as those with certain medical conditions or living in outbreak settings.
The CDC recommends a 2-dose primary series of MenACWY for individuals with conditions like complement deficiencies, asplenia, or HIV, followed by booster doses every 5 years.