Vaccinations do not fall into any drug schedule as classified by regulatory bodies such as the U.S. Drug Enforcement Administration (DEA) or similar organizations in other countries. Drug schedules are categories used to classify controlled substances based on their potential for abuse, medical use, and safety, typically ranging from Schedule I (high potential for abuse, no accepted medical use) to Schedule V (low potential for abuse, accepted medical use). Vaccines, on the other hand, are biological products regulated by health authorities like the U.S. Food and Drug Administration (FDA) or the World Health Organization (WHO), and are categorized separately due to their preventive nature and distinct regulatory pathways. They are subject to rigorous testing, approval, and monitoring to ensure safety and efficacy, but are not classified under controlled substance schedules.
Explore related products






What You'll Learn
![]()
Vaccines and Controlled Substances Act
Vaccines, unlike many pharmaceuticals, are not classified under the Controlled Substances Act (CSA) schedules. This might seem counterintuitive given the rigorous oversight vaccines undergo, but the CSA’s focus is on substances with potential for abuse or dependence. Vaccines, designed to stimulate immune responses rather than alter mental states or induce addiction, fall outside this scope. Instead, they are regulated under the Federal Food, Drug, and Cosmetic Act (FD&C Act) and the Public Health Service Act, which ensure safety, efficacy, and proper manufacturing practices. This distinction is critical for understanding how vaccines are legally categorized and managed in the United States.
The CSA’s scheduling system, ranging from Schedule I (high potential for abuse, no accepted medical use) to Schedule V (lowest potential for abuse), does not apply to vaccines because they do not meet the criteria for controlled substances. For example, opioids like morphine are Schedule II due to their high abuse potential and severe dependence liability, while cough syrups with limited codeine are Schedule V. Vaccines, such as the measles-mumps-rubella (MMR) or influenza vaccines, are biologics, not chemical compounds with psychoactive effects. Their regulation focuses on preventing contamination, ensuring consistent potency, and monitoring adverse events post-approval, tasks overseen by the FDA and CDC.
A practical takeaway for healthcare providers and the public is that vaccines’ exclusion from the CSA simplifies their distribution and administration. Unlike controlled substances, which require DEA registration, triplicate prescriptions, and strict inventory tracking, vaccines can be administered in various settings, from pediatric clinics to public health fairs. However, this does not mean vaccines are unregulated. The Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD) monitor safety, while the Advisory Committee on Immunization Practices (ACIP) provides dosage and scheduling guidelines. For instance, the COVID-19 mRNA vaccines received Emergency Use Authorization (EUA) or full approval with specific age-based dosing (e.g., 30 µg for Pfizer in adults, 10 µg for children 5–11).
Comparatively, the regulatory framework for vaccines aligns more closely with biologics like insulin or blood products than with controlled substances. This distinction is essential for policymakers and healthcare professionals to avoid confusion. While the CSA addresses drugs like fentanyl or benzodiazepines, vaccine oversight emphasizes population health and disease prevention. For parents or patients, understanding this difference can clarify why vaccines are widely accessible yet rigorously tested, unlike scheduled drugs, which face restrictions to curb misuse.
In conclusion, vaccines’ absence from the CSA schedules reflects their unique role in public health. Their regulation prioritizes safety and efficacy without the constraints of controlled substance laws. This system allows for broad accessibility while maintaining stringent quality control, ensuring vaccines remain a cornerstone of preventive medicine. For those administering or receiving vaccines, knowing this regulatory context underscores the balance between widespread availability and scientific oversight.
Bank by Mail Processing Time: What to Expect for Deposits
You may want to see also
Explore related products






![]()
FDA Classification of Vaccines
Vaccines, unlike many other medical products, are not classified under the standard drug scheduling system used by the FDA for controlled substances. This system, which categorizes drugs from Schedule I to Schedule V based on their potential for abuse and medical use, does not apply to vaccines. Instead, the FDA regulates vaccines under a distinct framework designed specifically for biological products, ensuring their safety, efficacy, and quality.
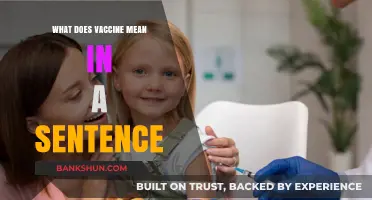
The FDA’s Center for Biologics Evaluation and Research (CBER) oversees vaccine approval and classification. Vaccines are classified based on their intended use, target population, and formulation. For instance, childhood vaccines like the MMR (measles, mumps, rubella) are categorized separately from adult vaccines such as the shingles vaccine (Shingrix). Each vaccine undergoes rigorous clinical trials to determine appropriate dosage, administration schedules, and age-specific recommendations. For example, the influenza vaccine is administered annually, while the HPV vaccine is given in a series of two or three doses, depending on the recipient’s age at the first dose.
One critical aspect of FDA vaccine classification is the distinction between routine and travel vaccines. Routine vaccines, such as those for tetanus or hepatitis B, are recommended for the general population and often included in immunization schedules. Travel vaccines, like yellow fever or typhoid, are reserved for specific populations based on geographic risk or occupational exposure. The FDA provides detailed guidelines for healthcare providers, including storage requirements (e.g., refrigeration at 2–8°C for most vaccines) and contraindications, such as severe allergies to vaccine components like egg proteins in the flu vaccine.
The FDA also classifies vaccines by their type, such as live attenuated (e.g., MMR), inactivated (e.g., polio), subunit (e.g., hepatitis B), or mRNA (e.g., COVID-19). This classification influences administration protocols, such as avoiding live vaccines in immunocompromised individuals. Additionally, the FDA monitors post-approval safety through systems like VAERS (Vaccine Adverse Event Reporting System), ensuring ongoing evaluation of risks and benefits.
Practical tips for healthcare providers include verifying patient-specific factors like age, pregnancy status, and medical history before administering vaccines. For example, the Tdap vaccine (tetanus, diphtheria, pertussis) is recommended during each pregnancy to protect newborns, while live vaccines are generally avoided in pregnant individuals. Understanding FDA classifications empowers providers to make informed decisions, ensuring vaccines are used safely and effectively across diverse populations.
Contacting Bank of Montreal: Easy Ways to Reach Customer Support
You may want to see also
Explore related products






![]()
Schedule Exemptions for Vaccines
Vaccines, unlike most drugs, are not classified under the standard drug scheduling systems such as the Controlled Substances Act in the United States or similar frameworks in other countries. This exemption is rooted in their unique purpose, safety profile, and regulatory oversight. While controlled substances are categorized based on their potential for abuse and medical use (e.g., Schedule I to V in the U.S.), vaccines are instead regulated under biologics licensing, ensuring they meet stringent safety, efficacy, and manufacturing standards. This distinction highlights their role as preventive tools rather than therapeutic agents with abuse potential.
The exemption of vaccines from drug schedules simplifies their distribution and administration, particularly in public health contexts. For instance, influenza vaccines are administered annually to millions without the need for prescriptions or controlled substance tracking. This streamlined approach is critical during outbreaks, where rapid deployment can save lives. However, it also necessitates robust monitoring systems, such as the Vaccine Adverse Event Reporting System (VAERS) in the U.S., to ensure ongoing safety. Unlike scheduled drugs, which may require specific storage or handling due to their controlled nature, vaccines are often stored in standard medical refrigerators, making them accessible even in remote settings.
From a regulatory perspective, vaccines are subject to a different set of rules that prioritize population health over individual prescription control. For example, childhood vaccines like the MMR (measles, mumps, rubella) are administered according to age-specific schedules, typically starting at 12–15 months with boosters at 4–6 years. This structured approach ensures herd immunity while avoiding the complexities of scheduling. Additionally, emergency use authorizations (EUAs) for vaccines, as seen during the COVID-19 pandemic, further illustrate their unique regulatory pathway, allowing rapid deployment without the constraints of controlled substance classification.
Practically, this exemption means healthcare providers can focus on education and accessibility rather than navigating bureaucratic hurdles. For parents, this translates to straightforward vaccination schedules for children, often provided at routine pediatric visits. Adults, too, benefit from simplified access to vaccines like Tdap (tetanus, diphtheria, pertussis) or shingles vaccines, which are recommended at specific ages (e.g., Tdap during pregnancy or shingles vaccine after age 50). This system underscores the balance between ensuring safety and promoting widespread immunization, a cornerstone of public health.
In conclusion, the exemption of vaccines from drug scheduling reflects their distinct role in preventive medicine and the regulatory frameworks designed to support their efficacy and accessibility. By avoiding the constraints of controlled substance classification, vaccines can be administered efficiently, saving lives and preventing disease on a global scale. This unique regulatory approach serves as a model for how public health tools can be optimized to meet societal needs.
Discover US Bank Rotating Categories for Maximum Rewards
You may want to see also
Explore related products




$28.99 $32.99

![International Certificate of Vaccination with Vinyl Document Holder - World Health Organization Bilingual Version [cards] World Health Organization [Jan 01, 2007]](https://m.media-amazon.com/images/I/61SHjBP1VYL._AC_UY218_.jpg)
![]()
Vaccines vs. Prescription Drugs
Vaccines and prescription drugs are both regulated by the FDA, but they fall into distinct categories under the Controlled Substances Act. Vaccines are not classified under any drug schedule because they are biological products designed to prevent diseases, not treat symptoms or alter physiological states. In contrast, prescription drugs are often categorized into Schedules II through V based on their potential for abuse, medical use, and safety profiles. For instance, opioids like oxycodone are Schedule II due to their high abuse potential, while cough suppressants with codeine are Schedule V, reflecting lower risk. This fundamental difference in classification underscores their unique roles in healthcare: vaccines are preventive measures, while prescription drugs are therapeutic interventions.
Consider the administration process: vaccines are typically given in standardized doses based on age and weight, such as the 0.5 mL dose of the Pfizer-BioNTech COVID-19 vaccine for individuals aged 12 and older. Prescription drugs, however, often require personalized dosing, like the 20–60 mg/day range for fluoxetine (an antidepressant), adjusted based on patient response and side effects. Vaccines are usually administered by healthcare professionals in controlled settings, whereas prescription drugs are often self-administered at home, necessitating clear instructions and patient education. This highlights the importance of adherence and monitoring for prescription drugs, which vaccines largely bypass due to their one-time or limited dosing schedules.
From a regulatory perspective, vaccines undergo rigorous testing for safety and efficacy before approval, but their post-market surveillance focuses on adverse events like anaphylaxis or rare complications. Prescription drugs, on the other hand, are continuously monitored for long-term effects, drug interactions, and misuse potential. For example, the CDC’s Vaccine Adverse Event Reporting System (VAERS) tracks vaccine side effects, while the FDA’s Adverse Event Reporting System (FAERS) monitors prescription drugs. This difference reflects the preventive nature of vaccines versus the ongoing therapeutic use of prescription drugs, which may require adjustments over time.
Practically, vaccines are often provided at no cost to patients in many countries, funded by public health programs to ensure widespread immunity. Prescription drugs, however, can be costly and may require insurance coverage or financial assistance programs. For instance, the shingles vaccine Shingrix is covered under Medicare Part D, while a month’s supply of insulin can cost hundreds of dollars without insurance. This disparity emphasizes the societal investment in prevention through vaccines versus the individual burden of managing chronic conditions with prescription drugs.
In summary, while both vaccines and prescription drugs are critical to public health, their regulatory classification, administration, monitoring, and cost structures differ significantly. Vaccines operate as preventive tools, unscheduled and universally dosed, while prescription drugs are therapeutic agents, scheduled based on risk, and tailored to individual needs. Understanding these distinctions helps patients and healthcare providers navigate their roles in maintaining health and treating disease effectively.
Exploring Banks Lake: Nearby Cities in Washington State Revealed
You may want to see also
Explore related products






![]()
Regulatory Oversight of Immunizations
Vaccinations, unlike many pharmaceuticals, do not fall into the standard drug scheduling system used for controlled substances. This system, established by the Controlled Substances Act, categorizes drugs based on their potential for abuse and medical use. Vaccines, however, are biological products primarily regulated by the Center for Biologics Evaluation and Research (CBER) within the FDA. This distinction is crucial because it reflects the unique nature of vaccines as preventative tools rather than therapeutic agents.
Understanding the Regulatory Landscape
The regulatory oversight of immunizations involves a multi-layered process ensuring safety, efficacy, and quality. It begins with pre-clinical testing, where potential vaccines are evaluated in laboratory and animal studies. This phase is critical for identifying any safety concerns before human trials commence. Following this, clinical trials are conducted in three phases, each progressively larger, to assess safety, immunogenicity, and efficacy in humans. These trials are closely monitored by regulatory bodies like the FDA, which scrutinize data for any adverse effects and ensure the vaccine meets stringent standards.
The Approval Process and Beyond
Once a vaccine demonstrates safety and efficacy in clinical trials, manufacturers submit a Biologics License Application (BLA) to the FDA. This application includes all data from pre-clinical and clinical studies, manufacturing information, and proposed labeling. The FDA’s CBER reviews the BLA, often consulting with advisory committees comprising independent experts. If approved, the vaccine is licensed for use, but oversight doesn’t end there. Post-market surveillance, including the Vaccine Adverse Event Reporting System (VAERS) and the Vaccine Safety Datalink (VSD), continuously monitors for rare or long-term side effects. This ongoing vigilance ensures that even after approval, vaccines remain safe for widespread use.
Practical Considerations for Healthcare Providers
Healthcare providers play a pivotal role in the administration of vaccines, adhering to guidelines set by regulatory bodies. For instance, the CDC’s Advisory Committee on Immunization Practices (ACIP) provides recommendations on vaccine use, including dosage, scheduling, and contraindications. For example, the MMR vaccine is typically administered in two doses, the first at 12-15 months of age and the second at 4-6 years. Providers must also be aware of storage requirements, as vaccines like the influenza vaccine often require refrigeration at 2-8°C. Proper handling and administration are essential to maintain vaccine efficacy and patient safety.
The Global Perspective
Is Macie Banks Still on the Highway? Latest Updates Revealed
You may want to see also
Frequently asked questions
Vaccinations do not fall into any of the drug schedules (Schedule I, II, III, IV, or V) as defined by the Controlled Substances Act. They are classified as biological products and regulated by the FDA under different guidelines.
No, vaccines are not considered controlled substances. They are regulated as biologics by the FDA and do not fall under the scheduling system for controlled substances.
While some vaccines may require a prescription or recommendation from a healthcare provider, this is unrelated to drug scheduling. Vaccines are not scheduled drugs and are regulated separately as biological products.
Vaccines are not included in the drug scheduling system because they are not controlled substances. The scheduling system is designed for drugs with potential for abuse or dependence, whereas vaccines are preventive biological products with a different regulatory framework.