Vaccines are essential tools in preventing infectious diseases, and they work by training the immune system to recognize and combat pathogens. Two prominent types of vaccines are mRNA vaccines and non-mRNA vaccines, each utilizing distinct mechanisms to achieve immunity. mRNA vaccines, such as those developed by Pfizer-BioNTech and Moderna for COVID-19, introduce genetic material (messenger RNA) that instructs cells to produce a harmless piece of the virus, triggering an immune response. In contrast, non-mRNA vaccines, like traditional inactivated or protein-based vaccines, directly deliver viral proteins or weakened/killed pathogens to stimulate immunity. Understanding the differences between these vaccine types is crucial for appreciating their efficacy, safety, and applications in modern medicine.
Explore related products






What You'll Learn
- mRNA Vaccines: Mechanism - mRNA teaches cells to produce viral proteins, triggering immune response without live virus
- Non-mRNA Vaccines: Types - Includes inactivated, live-attenuated, protein subunit, and viral vector vaccines
- Stability Differences - mRNA vaccines require ultra-cold storage; non-mRNA vaccines are more stable
- Immune Response - mRNA offers rapid, strong immunity; non-mRNA relies on traditional antigen presentation
- Development Speed - mRNA technology allows faster production; non-mRNA methods are slower, well-established
![]()
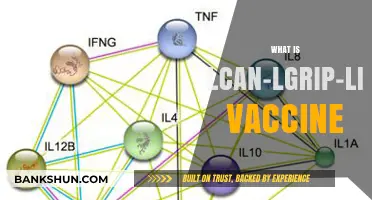
mRNA Vaccines: Mechanism - mRNA teaches cells to produce viral proteins, triggering immune response without live virus
MRNA vaccines represent a groundbreaking approach to immunization, leveraging the body's own cellular machinery to mount a defense against pathogens. Unlike traditional vaccines that introduce a weakened or inactivated virus, mRNA vaccines deliver a genetic blueprint—a messenger RNA (mRNA) sequence—that instructs cells to produce a harmless piece of the virus, typically a spike protein. This process mimics viral infection without the risk of causing disease, as the mRNA does not alter human DNA and degrades quickly after use. For instance, the Pfizer-BioNTech and Moderna COVID-19 vaccines use this technology, requiring two doses administered 3–4 weeks apart for optimal immunity in individuals aged 12 and older.
The mechanism begins when the mRNA is encased in lipid nanoparticles, which protect it during transit and facilitate entry into muscle cells at the injection site. Once inside, the mRNA hijacks the cell’s ribosomes, the protein-making factories, to synthesize the viral protein. This protein is then displayed on the cell’s surface, flagging it for immune system recognition. Antigen-presenting cells, such as dendritic cells, engulf the protein and transport it to lymph nodes, where they activate T cells and B cells. B cells produce antibodies tailored to neutralize the viral protein, while T cells prepare to destroy any infected cells, creating a robust and memory-based immune response.
One of the key advantages of mRNA vaccines is their precision and safety. Since they do not contain live virus, they eliminate the risk of infection or reversion to a virulent form, making them suitable for immunocompromised individuals. Additionally, mRNA vaccines can be rapidly developed and scaled, as seen during the COVID-19 pandemic, where they were produced within months of identifying the SARS-CoV-2 genome. However, their storage requirements—ultra-cold temperatures for some formulations—pose logistical challenges, particularly in low-resource settings.
Practical considerations for mRNA vaccination include adhering to the recommended dosage schedule and monitoring for rare side effects, such as myocarditis, which has been observed primarily in young males after the second dose. Recipients should stay hydrated and plan for potential mild to moderate symptoms, such as fatigue, headache, or injection site pain, which typically resolve within 48 hours. For those with a history of severe allergic reactions, consultation with a healthcare provider is advised before vaccination.
In comparison to non-mRNA vaccines, such as viral vector (e.g., Johnson & Johnson) or protein subunit (e.g., Novavax) vaccines, mRNA vaccines offer higher efficacy rates, often exceeding 90% after full dosing. Their ability to elicit both humoral and cellular immunity positions them as a versatile platform for combating emerging pathogens. As research advances, mRNA technology holds promise for addressing other diseases, including influenza, HIV, and cancer, marking a new era in vaccinology.
Mastering Intraday Bank Nifty Trading: Strategies, Tips, and Techniques
You may want to see also
Explore related products






![]()
Non-mRNA Vaccines: Types - Includes inactivated, live-attenuated, protein subunit, and viral vector vaccines
Non-mRNA vaccines have been the backbone of immunization for decades, relying on established technologies that deliver antigens to the immune system without genetic material. Among these, inactivated vaccines stand out for their safety and stability. Created by killing the pathogen (e.g., polio, hepatitis A) with chemicals or heat, these vaccines cannot cause disease but still provoke an immune response. For instance, the inactivated polio vaccine (IPV) is administered as a series of four doses starting at 2 months of age, offering robust protection without the risk of vaccine-derived polio. However, multiple doses are often required to achieve lasting immunity, as the immune response is typically weaker than with live vaccines.
In contrast, live-attenuated vaccines use a weakened form of the virus or bacteria (e.g., measles, mumps, rubella in the MMR vaccine) to mimic natural infection. This approach triggers a strong, long-lasting immune response, often requiring just one or two doses. For example, the MMR vaccine is given in two doses, the first at 12–15 months and the second at 4–6 years. While highly effective, live vaccines carry a small risk of causing mild disease in immunocompromised individuals, making them unsuitable for certain populations. Their ability to replicate in the body ensures a robust immune memory, but storage and transport require refrigeration to maintain viability.
Protein subunit vaccines take a more precise approach by using only specific pieces of the pathogen, such as proteins or sugars, to stimulate immunity. The hepatitis B vaccine, for instance, contains only the virus’s surface antigen (HBsAg), eliminating any risk of infection. This type is ideal for those with weakened immune systems, as it cannot cause disease. However, adjuvants (e.g., aluminum salts) are often added to enhance the immune response, and multiple doses may be needed. The HPV vaccine (Gardasil 9) is another example, protecting against nine strains of human papillomavirus with just three doses over 6 months.
Viral vector vaccines represent a newer category, leveraging a harmless virus (the vector) to deliver genetic material encoding a pathogen’s antigen. Unlike mRNA vaccines, the genetic material does not enter the cell nucleus. The Johnson & Johnson COVID-19 vaccine, for example, uses an adenovirus vector to deliver instructions for producing the SARS-CoV-2 spike protein. This single-dose vaccine offers flexibility in storage (refrigerated temperatures) and is particularly useful in resource-limited settings. However, rare side effects, such as thrombosis with thrombocytopenia syndrome (TTS), have been reported, primarily in younger women, highlighting the need for careful patient selection.
Each non-mRNA vaccine type has unique advantages and limitations, tailored to specific pathogens and populations. Inactivated and subunit vaccines excel in safety, making them suitable for vulnerable groups, while live-attenuated vaccines provide unmatched durability. Viral vector vaccines combine the benefits of genetic approaches with traditional delivery methods, offering a middle ground. Understanding these distinctions empowers healthcare providers and individuals to make informed decisions, ensuring the right vaccine for the right context.
Kaiser's Role in Monkeypox Vaccination: Availability and Eligibility Explained
You may want to see also
Explore related products






![]()
Stability Differences - mRNA vaccines require ultra-cold storage; non-mRNA vaccines are more stable
One of the most striking differences between mRNA and non-mRNA vaccines is their storage requirements. mRNA vaccines, such as Pfizer-BioNTech and Moderna’s COVID-19 offerings, demand ultra-cold temperatures—Pfizer’s must be stored at -94°F (-70°C), while Moderna’s can tolerate -13°F (-25°C) for long-term storage. This fragility stems from the mRNA molecule’s susceptibility to degradation when exposed to heat, light, or enzymes. In contrast, non-mRNA vaccines, like AstraZeneca’s viral vector or Novavax’s protein subunit vaccines, remain stable at standard refrigerator temperatures (36°F–46°F or 2°C–8°C). This disparity isn’t just a logistical detail—it shapes accessibility, especially in low-resource settings where ultra-cold chains are impractical.
Consider the practical implications for healthcare providers. Administering mRNA vaccines requires specialized freezers, dry ice shipments, and meticulous handling to maintain efficacy. For instance, Pfizer’s vaccine can only be stored at room temperature for up to 2 hours post-thaw, while Moderna’s allows a 12-hour window. Non-mRNA vaccines, however, offer flexibility. AstraZeneca’s vaccine, for example, can be stored for up to 6 months in a standard fridge, simplifying distribution in rural or remote areas. This stability difference directly impacts vaccination campaigns, particularly in regions with unreliable electricity or limited infrastructure.
From a cost perspective, the stability gap translates to significant financial burdens. Ultra-cold storage equipment can cost tens of thousands of dollars per unit, not including maintenance and energy expenses. Developing nations often face a stark choice: invest heavily in cold chain infrastructure or opt for more stable non-mRNA alternatives. For instance, India’s widespread use of the Oxford-AstraZeneca vaccine (stored at 2°C–8°C) was pivotal in its mass vaccination efforts, whereas mRNA vaccines were reserved for specific populations due to storage constraints. This economic divide underscores the stability advantage of non-mRNA vaccines in global health equity discussions.
Despite these challenges, mRNA vaccines’ ultra-cold requirements aren’t insurmountable. Innovations like lipid nanoparticle encapsulation and lyophilization (freeze-drying) are being explored to enhance mRNA stability. Moderna’s recent trials suggest a next-generation vaccine stable at 36°F–46°F, potentially bridging the gap. However, until such advancements become standard, non-mRNA vaccines retain their edge in stability. For now, healthcare systems must weigh the benefits of mRNA’s rapid development and high efficacy against the logistical simplicity of non-mRNA options, particularly in resource-constrained environments.
Understanding EDD: What Does EDD Stand for in Banking Compliance?
You may want to see also
Explore related products






![]()
Immune Response - mRNA offers rapid, strong immunity; non-mRNA relies on traditional antigen presentation
The immune system's response to vaccines is a critical factor in their effectiveness, and the mechanism by which this response is triggered differs significantly between mRNA and non-mRNA vaccines. mRNA vaccines, such as Pfizer-BioNTech and Moderna's COVID-19 vaccines, introduce a genetic code that instructs cells to produce a specific viral protein, typically the spike protein. This process begins almost immediately upon injection, with the mRNA entering cells within hours. The immune system recognizes this protein as foreign, prompting a rapid and robust response, including the production of antibodies and activation of T cells. For instance, studies show that the Pfizer vaccine achieves peak antibody levels around 7 days after the second dose, offering up to 95% efficacy in preventing symptomatic COVID-19 in individuals aged 16 and older.
In contrast, non-mRNA vaccines, like the Oxford-AstraZeneca and Johnson & Johnson COVID-19 vaccines, rely on traditional antigen presentation. These vaccines deliver either a weakened or inactivated virus, or a viral vector carrying genetic material, to introduce the antigen directly. The immune response is slower because the antigen must be processed by antigen-presenting cells (APCs) before it can trigger an immune reaction. For example, the Oxford-AstraZeneca vaccine, which uses a chimpanzee adenovirus vector, typically requires 2–3 weeks after the second dose to reach peak efficacy, which is around 76% in preventing symptomatic COVID-19. This delay is due to the additional steps required for APCs to process and present the antigen to immune cells.
One practical advantage of mRNA vaccines is their ability to induce a strong memory response with lower antigen doses. For instance, the Moderna vaccine uses a 100-microgram dose for the initial series, while the Pfizer vaccine uses 30 micrograms. Non-mRNA vaccines often require higher antigen loads or adjuvants to achieve comparable immunity. The Johnson & Johnson vaccine, a single-dose adenovirus vector vaccine, uses a full viral particle to deliver the antigen, yet still achieves only around 66% efficacy in preventing moderate to severe COVID-19 globally. This highlights the trade-off between rapid, high-efficacy responses with mRNA vaccines and the more gradual, traditional immune activation of non-mRNA options.
For individuals considering vaccination, understanding these differences can guide decision-making. mRNA vaccines are ideal for those seeking rapid protection, particularly in high-transmission settings. However, they require ultra-cold storage, which can limit accessibility in certain regions. Non-mRNA vaccines, while slower to act, are more logistically feasible and may be preferred for populations with limited access to advanced medical infrastructure. For example, the Oxford-AstraZeneca vaccine can be stored at standard refrigerator temperatures (2–8°C), making it a practical choice for low-resource areas.
In summary, mRNA vaccines leverage cellular machinery to produce antigens swiftly, triggering a rapid and potent immune response. Non-mRNA vaccines depend on traditional antigen processing, resulting in a slower but still effective immune activation. Both approaches have unique strengths, and the choice between them should consider factors like urgency of protection, logistical constraints, and individual health needs. For instance, a young, healthy adult in an urban area might opt for an mRNA vaccine for quick immunity, while a rural community with limited refrigeration might prioritize a non-mRNA option. Tailoring the vaccine choice to these specifics ensures optimal immune response and practical feasibility.
Parker Posey and Elizabeth Banks: Unraveling the Family Connection Myth
You may want to see also
Explore related products






![]()
Development Speed - mRNA technology allows faster production; non-mRNA methods are slower, well-established
The COVID-19 pandemic spotlighted a critical difference between mRNA and non-mRNA vaccines: development speed. mRNA vaccines, like Pfizer-BioNTech and Moderna, were authorized for emergency use within a year of the pandemic's onset. This unprecedented pace was possible because mRNA technology relies on synthesizing genetic material encoding a viral protein, a process that can be rapidly adapted to new pathogens. In contrast, non-mRNA vaccines, such as AstraZeneca’s viral vector and Novavax’s protein subunit vaccines, took longer to develop due to the need to cultivate, purify, or engineer specific viral components, often requiring established but time-consuming manufacturing processes.
Consider the steps involved in producing these vaccines. mRNA vaccines begin with identifying the target antigen (e.g., the SARS-CoV-2 spike protein), sequencing its genetic code, and synthesizing mRNA molecules. This process can be completed in weeks, and scaling up production involves replicating the same mRNA sequence. Non-mRNA methods, however, often require growing viruses or bacteria in bioreactors, purifying proteins, or engineering cells to produce viral components—steps that can take months. For instance, Novavax’s vaccine relies on insect cells to produce the spike protein, a process that, while reliable, is slower than mRNA synthesis.
The speed of mRNA technology offers a strategic advantage during outbreaks. During the H1N1 swine flu pandemic in 2009, non-mRNA vaccines took approximately six months to develop and distribute, leaving populations vulnerable during the initial wave. mRNA’s rapid turnaround could have significantly reduced this timeline. However, this speed comes with a trade-off: mRNA vaccines require ultra-cold storage (e.g., -70°C for Pfizer’s vaccine), which poses logistical challenges, especially in low-resource settings. Non-mRNA vaccines, like AstraZeneca’s, can be stored at standard refrigerator temperatures (2–8°C), making distribution simpler.
Despite mRNA’s speed, non-mRNA methods remain valuable due to their established track record. Vaccines like the flu shot and hepatitis B vaccine have been refined over decades, providing long-term safety and efficacy data. mRNA technology, while promising, is relatively new, with COVID-19 vaccines being the first mRNA products approved for human use. For example, the flu vaccine is updated annually based on circulating strains, a process that leverages well-established non-mRNA techniques. This reliability makes non-mRNA vaccines a cornerstone of public health, even if they lag in development speed.
In practice, the choice between mRNA and non-mRNA vaccines depends on the context. During a rapidly spreading pandemic, mRNA’s speed is invaluable, but for routine immunizations, non-mRNA vaccines’ stability and ease of distribution may be preferable. For instance, a child receiving a standard immunization schedule might get non-mRNA vaccines for measles or polio, while an adult during a pandemic might opt for an mRNA COVID-19 booster. Understanding these differences empowers individuals and policymakers to make informed decisions, balancing urgency with practicality.
JetBlue Travel Bank Expiration: How Long Do Credits Last?
You may want to see also
Frequently asked questions
mRNA vaccines (like Pfizer-BioNTech and Moderna) use messenger RNA to instruct cells to produce a harmless piece of the virus (e.g., the spike protein of SARS-CoV-2), triggering an immune response. Non-mRNA vaccines, such as viral vector (e.g., Johnson & Johnson) or protein subunit (e.g., Novavax) vaccines, use different methods to deliver viral components or proteins directly to the immune system without involving mRNA.
Both mRNA and non-mRNA vaccines are highly effective in preventing severe illness, hospitalization, and death from diseases like COVID-19. However, mRNA vaccines have shown slightly higher efficacy rates in clinical trials compared to some non-mRNA vaccines. The choice depends on availability, individual health conditions, and specific vaccine recommendations.
Side effects can vary between mRNA and non-mRNA vaccines. mRNA vaccines commonly cause temporary side effects like fatigue, headache, and muscle pain at the injection site. Non-mRNA vaccines, such as viral vector vaccines, may cause side effects like fever, nausea, or rare cases of blood clots. It’s important to consult a healthcare provider to understand which vaccine is best for you.