Vaccines provide active, adaptive immunity by training the body’s immune system to recognize and combat specific pathogens without causing the disease itself. They achieve this by introducing a harmless form of the pathogen (such as a weakened or inactivated virus, a protein fragment, or genetic material) to stimulate the production of antibodies and memory cells. This prepares the immune system to mount a rapid and effective response if the real pathogen is encountered in the future. The immunity conferred by vaccines can be short-term or long-term, depending on the vaccine type and the pathogen, and may require booster doses to maintain protection. While vaccines primarily protect individuals, they also contribute to herd immunity when a large portion of the population is vaccinated, reducing the spread of disease and protecting vulnerable individuals who cannot be vaccinated.
| Characteristics | Values |
|---|---|
| Type of Immunity | Active immunity (stimulates the body’s immune system to produce antibodies and memory cells) |
| Duration | Varies by vaccine; can be short-term (e.g., flu vaccine) or long-term (e.g., measles vaccine) |
| Specificity | Targeted to specific pathogens or antigens (e.g., COVID-19, influenza, tetanus) |
| Mechanism | Induces production of antibodies, B cells, and T cells for future protection |
| Natural vs. Vaccine-Induced | Mimics natural immunity but without the risk of severe disease from infection |
| Herd Immunity Contribution | Reduces disease spread by increasing population-level immunity |
| Booster Requirements | Some vaccines require boosters to maintain immunity (e.g., tetanus, COVID-19) |
| Efficacy | Varies by vaccine; typically 50–95% depending on the disease and vaccine type |
| Side Effects | Generally mild (e.g., soreness, fever) compared to natural infection risks |
| Adaptive Response | Trains the immune system to recognize and respond faster to future exposures |
| Passive Immunity | Not provided by vaccines; passive immunity is short-term and comes from antibodies (e.g., maternal antibodies) |
| Cross-Protection | Some vaccines offer partial protection against related strains (e.g., COVID-19 variants) |
| Age-Specific Responses | Immunity may vary by age group (e.g., weaker response in older adults) |
| Global Impact | Eradicated diseases like smallpox and reduced prevalence of others (e.g., polio) |
Explore related products






What You'll Learn
![]()
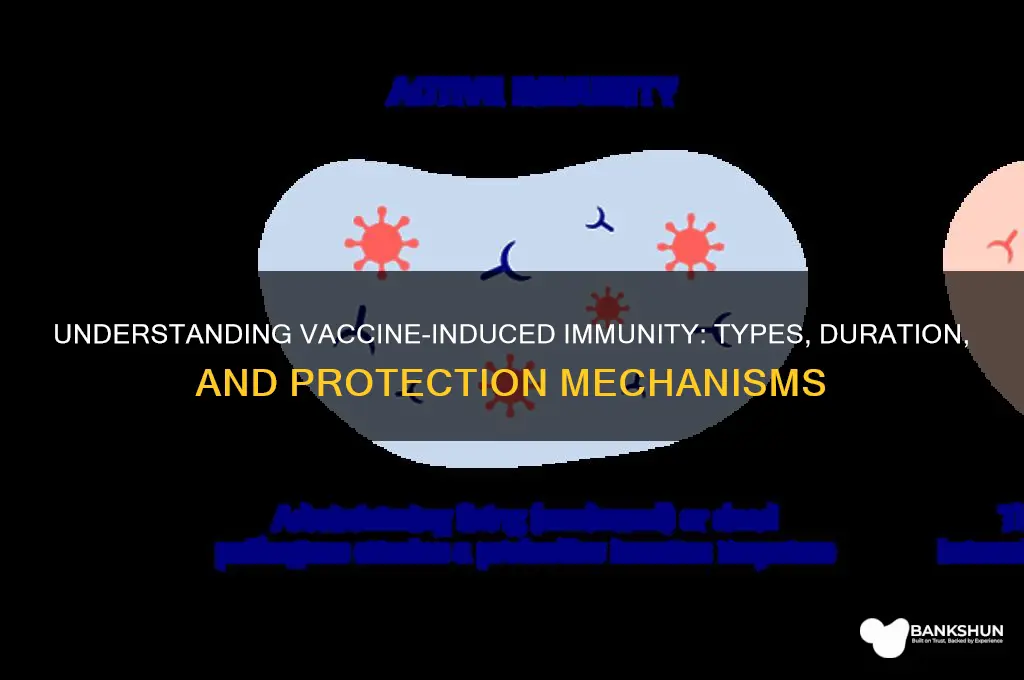
Active vs. Passive Immunity
Vaccines harness the body’s immune system to prevent disease, but they don’t all work the same way. The key distinction lies in whether they trigger active immunity or provide passive immunity. Active immunity occurs when the immune system is stimulated to produce its own antibodies, typically through vaccination with weakened or inactivated pathogens. For example, the measles, mumps, and rubella (MMR) vaccine introduces a harmless form of the viruses, prompting the body to create memory cells that recognize and combat future infections. This process takes time—usually weeks—but the resulting immunity can last decades or even a lifetime. In contrast, passive immunity involves the direct transfer of pre-made antibodies, such as those found in the DTaP vaccine for diphtheria, tetanus, and pertussis, which offers immediate but short-term protection, often lasting only weeks to months.
Consider the scenario of a newborn exposed to whooping cough. Since their immune system is immature, they cannot yet receive the full DTaP vaccine series. Instead, their mother can receive a Tdap booster during pregnancy, transferring protective antibodies across the placenta. This is passive immunity in action—rapid but temporary. Active immunity, however, is the cornerstone of long-term prevention. For instance, the two-dose HPV vaccine series (administered 6–12 months apart) trains the immune system to recognize human papillomavirus, reducing the risk of cervical cancer by over 90% in vaccinated individuals. The timing and dosage of these vaccines are critical; the HPV vaccine is recommended for adolescents aged 11–12, as earlier immunization maximizes immune response.
While active immunity is the gold standard for durable protection, passive immunity plays a vital role in specific situations. For example, individuals exposed to rabies receive both a rabies vaccine (active immunity) and rabies immunoglobulin (passive immunity). The vaccine primes the immune system over several weeks, while the immunoglobulin provides immediate antibodies to neutralize the virus. This dual approach is life-saving, as rabies is nearly 100% fatal once symptoms appear. Similarly, monoclonal antibody treatments for COVID-19 offer passive immunity to high-risk individuals, though their protection wanes within months, underscoring the limitations of this approach compared to active immunity from vaccines like Pfizer or Moderna.
The choice between active and passive immunity depends on context. Active immunity is ideal for long-term prevention, as seen in the annual flu vaccine, which requires yearly updates due to viral mutations but still reduces severe illness by 40–60%. Passive immunity, however, is indispensable in emergencies or for immunocompromised individuals who cannot mount a robust response to vaccines. For instance, infants under 6 months old are too young for the flu vaccine but can benefit from maternal antibodies if their mother was vaccinated during pregnancy. Understanding these differences empowers individuals to make informed decisions about vaccination, balancing immediate needs with long-term protection.
In practice, combining active and passive strategies can optimize outcomes. For travelers visiting regions with high hepatitis A risk, a single dose of immune globulin provides instant protection, while the hepatitis A vaccine, administered concurrently, ensures long-term immunity after two doses spaced 6–12 months apart. This hybrid approach illustrates the synergy between the two types of immunity. Ultimately, vaccines are not one-size-fits-all; they are tailored tools that leverage active or passive mechanisms—or both—to safeguard health. By recognizing their unique roles, we can better navigate the complexities of disease prevention in diverse populations.
How to Stop Autopay in Axis Bank: A Step-by-Step Guide
You may want to see also
Explore related products

$12.89 $13.99
$25.46 $27.98



![]()
Humoral vs. Cell-Mediated Responses
Vaccines harness the body’s immune system to provide protection against pathogens, but the type of immunity they elicit depends on the mechanism of action. At the core of this process lies the distinction between humoral and cell-mediated responses, two arms of the adaptive immune system. Humoral immunity, driven by B cells, produces antibodies that neutralize pathogens in the bloodstream and extracellular spaces. Cell-mediated immunity, orchestrated by T cells, targets infected cells and intracellular pathogens. Vaccines like the flu shot primarily stimulate humoral responses, while others, such as the BCG vaccine for tuberculosis, emphasize cell-mediated immunity. Understanding this duality is crucial for designing vaccines tailored to specific diseases.
Consider the measles vaccine, a live-attenuated virus that triggers both humoral and cell-mediated responses. B cells produce neutralizing antibodies that prevent the virus from infecting cells, while cytotoxic T cells identify and destroy infected cells. This dual action ensures robust protection, with efficacy rates exceeding 95% after two doses. In contrast, the hepatitis B vaccine relies heavily on humoral immunity, generating high levels of antibodies to block viral entry. However, vaccines like the COVID-19 mRNA vaccines (e.g., Pfizer-BioNTech) stimulate both pathways, with antibodies neutralizing the virus and T cells targeting infected cells. This versatility highlights the importance of tailoring vaccine design to the pathogen’s behavior.
To illustrate the practical implications, compare the tetanus toxoid vaccine and the shingles vaccine. Tetanus toxoid induces humoral immunity by generating antibodies against the toxin produced by *Clostridium tetani*. A single dose provides protection for 5–10 years, but boosters are required to maintain antibody levels. Conversely, the shingles vaccine (Shingrix) focuses on cell-mediated immunity, activating T cells to combat the varicella-zoster virus. Its two-dose regimen, administered 2–6 months apart, achieves over 90% efficacy in adults over 50, a population with waning immunity. This example underscores how vaccine efficacy hinges on aligning the immune response with the pathogen’s characteristics.
A critical takeaway is that some vaccines can shift the balance between humoral and cell-mediated responses based on dosage, formulation, or delivery method. For instance, adjuvants like aluminum salts in the HPV vaccine enhance humoral immunity by promoting antibody production. In contrast, viral vector vaccines (e.g., Johnson & Johnson’s COVID-19 vaccine) prioritize cell-mediated immunity by delivering genetic material directly into cells, prompting a T cell response. Clinicians and researchers must consider these nuances when recommending vaccines, especially for immunocompromised individuals or those with specific vulnerabilities.
In practice, understanding humoral vs. cell-mediated responses empowers individuals to make informed decisions about vaccination. For example, travelers to regions with high malaria risk might prioritize vaccines that stimulate cell-mediated immunity, as the parasite resides within red blood cells. Similarly, older adults should opt for vaccines like Shingrix that bolster T cell activity to counteract age-related immune decline. By recognizing the unique contributions of each immune pathway, we can maximize vaccine efficacy and tailor immunization strategies to individual needs.
Step-by-Step Guide to Applying for Standard Bank Learnership Program
You may want to see also
Explore related products






![]()
Duration of Vaccine-Induced Protection
Vaccines are designed to provide immunity, but the duration of this protection varies widely depending on the vaccine and the individual. For instance, the measles, mumps, and rubella (MMR) vaccine offers lifelong immunity after two doses, administered at 12–15 months and 4–6 years of age. In contrast, the tetanus vaccine requires booster shots every 10 years to maintain protection. Understanding these differences is crucial for effective immunization strategies, as it influences scheduling, public health policies, and individual compliance.
The duration of vaccine-induced protection is influenced by multiple factors, including the type of vaccine, the pathogen it targets, and the recipient’s immune system. Live-attenuated vaccines, like the MMR and varicella (chickenpox) vaccines, often provide long-lasting immunity because they mimic natural infection, stimulating a robust immune memory. Inactivated or subunit vaccines, such as the hepatitis B or influenza vaccines, typically require multiple doses or boosters to sustain protection. For example, the influenza vaccine is administered annually due to the virus’s rapid mutation and the waning of antibody levels over time.
Age plays a significant role in the duration of vaccine-induced immunity. Children and young adults generally mount stronger immune responses, leading to longer-lasting protection. However, immune function declines with age, a phenomenon known as immunosenescence, which can reduce the effectiveness and duration of vaccine-induced immunity in older adults. For instance, the shingles vaccine (Shingrix) is recommended for adults over 50, with two doses administered 2–6 months apart, to compensate for age-related immune decline.
Practical tips can help maximize the duration of vaccine-induced protection. Adhering to recommended vaccination schedules is essential, as delays or missed doses can compromise immunity. Keeping a vaccination record ensures timely boosters, especially for vaccines like tetanus or HPV, which require specific intervals between doses. For travelers, consulting a healthcare provider about destination-specific vaccines (e.g., yellow fever or typhoid) and their duration of protection is critical. Lastly, maintaining a healthy lifestyle—adequate sleep, nutrition, and exercise—supports overall immune function, potentially enhancing vaccine efficacy and longevity.
In summary, the duration of vaccine-induced protection is not one-size-fits-all but depends on vaccine type, pathogen characteristics, and individual factors like age and immune health. Tailoring vaccination strategies to these variables ensures optimal and sustained immunity. Whether it’s lifelong protection from the MMR vaccine or annual flu shots, understanding these nuances empowers individuals and healthcare providers to make informed decisions, ultimately strengthening public health defenses.
Understanding Meningococcal Vaccine Type B ACYW: Benefits, Uses, and Importance
You may want to see also
Explore related products






![]()
Herd Immunity Mechanisms
Vaccines don't just protect individuals; they weave a protective net around entire communities through a phenomenon known as herd immunity. This mechanism hinges on a critical threshold: when a sufficient proportion of a population becomes immune to a disease, either through vaccination or prior infection, the spread of the pathogen is significantly hindered. For highly contagious diseases like measles, this threshold can be as high as 95% immunity to disrupt transmission chains effectively.
Herd immunity operates through a simple yet powerful principle: pathogens require susceptible hosts to survive and propagate. When a large enough segment of the population is immune, the likelihood of a susceptible person coming into contact with an infected individual decreases dramatically. This interruption in the chain of infection effectively starves the pathogen of new hosts, leading to a decline in disease prevalence.
Achieving herd immunity requires strategic vaccination campaigns tailored to the specific disease and population demographics. For instance, the measles vaccine, typically administered in two doses (the first at 12-15 months and the second at 4-6 years), aims to reach the aforementioned 95% immunity threshold. However, maintaining this threshold is crucial, as even small pockets of unvaccinated individuals can create vulnerabilities, allowing outbreaks to occur. This is particularly concerning for diseases like pertussis (whooping cough), where immunity wanes over time, necessitating booster shots for adolescents and adults.
Herd immunity isn't merely a theoretical concept; its impact is evident in the eradication of smallpox and the near-elimination of polio in many regions. These successes underscore the power of collective action in disease prevention. However, challenges remain, including vaccine hesitancy, inequitable access to vaccines, and the emergence of new variants that can evade existing immunity.
To strengthen herd immunity, public health efforts must focus on increasing vaccine uptake through education, addressing access barriers, and promoting vaccine confidence. This includes dispelling misinformation, ensuring vaccines are affordable and accessible, and tailoring communication strategies to diverse communities. By working together, we can harness the power of herd immunity to protect not only ourselves but also the most vulnerable members of society.
Choosing the Right Vaccine: Which Brand Offers Optimal Protection?
You may want to see also
Explore related products






![]()
Memory Cell Formation Process
Vaccines harness the body’s ability to form memory cells, a cornerstone of long-term immunity. When a vaccine introduces a weakened or inactivated pathogen, the immune system responds by activating B and T lymphocytes. Among these, a subset of cells undergoes differentiation into memory cells, which persist long after the initial threat is neutralized. This process ensures that upon re-exposure to the same pathogen, the immune system can mount a rapid and robust response, often preventing illness altogether. For instance, the measles vaccine induces memory cells that remain viable for decades, providing lifelong protection in 95% of recipients after two doses.
The formation of memory cells begins with antigen presentation, where dendritic cells process vaccine antigens and display them to naive T cells in lymph nodes. This interaction triggers T cell proliferation and differentiation into effector and memory T cells. Simultaneously, B cells activated by the antigen mature into plasma cells, which secrete antibodies, and memory B cells. The survival of these memory cells depends on signals from cytokines and interactions with follicular helper T cells. Notably, adjuvants in vaccines, such as aluminum salts or mRNA lipid nanoparticles, enhance this process by prolonging antigen exposure and amplifying immune signals, as seen in the Pfizer-BioNTech COVID-19 vaccine, where a 30-microgram dose optimizes memory cell formation.
Memory cells are not uniform; they differentiate into distinct subsets with specialized functions. For example, effector memory T cells (TEM) circulate in the bloodstream and tissues, ready to quickly eliminate pathogens, while central memory T cells (TCM) reside in lymphoid organs, ensuring long-term immunity by self-renewal and replenishing TEM populations. Similarly, memory B cells localize to the bone marrow or lymph nodes, where they can rapidly differentiate into antibody-secreting plasma cells upon re-exposure. This diversity ensures that the immune response is both swift and sustained, as demonstrated by the tetanus vaccine, which requires booster doses every 10 years to maintain sufficient memory cell populations.
Practical considerations for optimizing memory cell formation include adhering to recommended vaccine schedules, as spacing doses (e.g., 4–8 weeks apart for the COVID-19 mRNA vaccines) allows time for memory cell maturation. Age also plays a role; infants and older adults may require additional doses or adjuvanted formulations due to less efficient immune responses. For example, the shingles vaccine (Shingrix) uses a recombinant protein and adjuvant system to enhance memory cell formation in individuals over 50, achieving over 90% efficacy. Avoiding immunosuppressive medications or behaviors (e.g., chronic sleep deprivation) around vaccination can further support this process.
In summary, memory cell formation is a dynamic, multi-step process central to vaccine-induced immunity. By understanding its mechanisms and practical implications, individuals and healthcare providers can maximize the protective benefits of vaccination. From antigen presentation to memory cell subset differentiation, each stage is critical for ensuring a durable immune response. Whether through precise dosing, adjuvant use, or adherence to schedules, optimizing this process remains key to public health strategies against infectious diseases.
Exploring the Existence of CTI Bank: Fact or Fiction?
You may want to see also
Frequently asked questions
Vaccines provide active immunity, which means they stimulate the body’s immune system to produce antibodies and memory cells to fight off specific pathogens.
In many cases, vaccines provide long-lasting immunity, but the duration varies depending on the vaccine and the individual. Some vaccines require booster shots to maintain protection.
No, vaccines typically take a few weeks to build immunity as the body needs time to produce antibodies and develop immune memory after vaccination.
Yes, when a large portion of a population is vaccinated, it can create herd immunity, reducing the spread of disease and protecting those who cannot be vaccinated.
Vaccines are designed to target specific strains or components of a virus. While they may offer some cross-protection against variants, effectiveness can vary depending on how different the variant is from the original target.