The global effort to eradicate polio has been a remarkable public health achievement, but it’s often overlooked that the disease was nearly eliminated in some regions even before the introduction of the polio vaccine in 1955. In the early 20th century, improved sanitation, hygiene, and public health measures significantly reduced polio cases in developed countries, leading to a decline in outbreaks. For instance, in the United States, polio incidence had already dropped by nearly 50% in the decade preceding the vaccine’s rollout. This pre-vaccine progress raises intriguing questions about the interplay between environmental factors, societal changes, and medical interventions in combating infectious diseases. However, the vaccine’s development ultimately proved essential in sustaining and accelerating the global eradication effort, as it provided a direct and scalable solution to prevent the virus’s spread.
| Characteristics | Values |
|---|---|
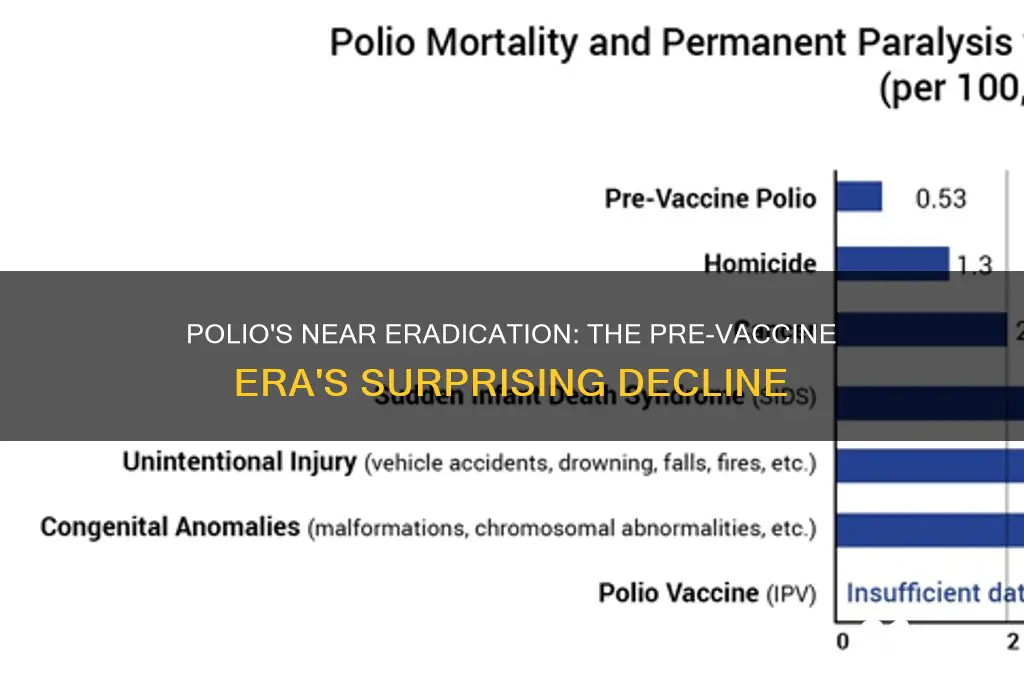
| Pre-vaccine Polio Incidence (1950s) | High; hundreds of thousands of cases annually worldwide |
| Natural Decline Before Vaccine | No significant decline; outbreaks were frequent and unpredictable |
| Sanitation and Hygiene Impact | Improved sanitation reduced some diseases but had minimal impact on polio transmission |
| Iron Lung Usage | Widespread use in the 1940s and 1950s to assist polio patients with paralyzed respiratory muscles |
| Public Fear and Awareness | High; polio was a major public health concern, especially in developed countries |
| Scientific Understanding | Limited; the virus and its transmission were not fully understood until the mid-20th century |
| Eradication Efforts Pre-Vaccine | Nonexistent; no coordinated global efforts to eradicate polio before the vaccine |
| Vaccine Development | Jonas Salk’s inactivated polio vaccine (IPV) introduced in 1955; Sabin’s oral polio vaccine (OPV) in 1961 |
| Post-Vaccine Decline | Dramatic reduction in cases; near-eradication achieved by 2000s |
| Current Status (2023) | Polio remains endemic in only 2 countries (Afghanistan and Pakistan); 99.9% reduction since 1988 |
| Conclusion | Polio was not almost eradicated before the vaccine; the vaccine was the primary driver of its near-eradication |
Explore related products






What You'll Learn
![]()
Pre-vaccine polio decline causes
Polio incidence began declining significantly in many developed countries before the introduction of vaccines in the 1950s. This trend raises questions about the factors driving the pre-vaccine decline, which are often overshadowed by the vaccine’s success. Improved sanitation and hygiene played a pivotal role, as polio is primarily transmitted through fecal-oral routes. In the early 20th century, public health initiatives focused on clean water supplies, sewage systems, and personal cleanliness, reducing exposure to the poliovirus in industrialized nations. For instance, the United States saw a 47% decrease in polio cases between 1923 and 1952, prior to widespread vaccination, correlating with major sanitation improvements during this period.
Another critical factor was the changing age distribution of polio infections. In the late 19th and early 20th centuries, polio primarily affected infants and young children, who often experienced mild or asymptomatic infections, building natural immunity in the population. However, as sanitation improved, fewer children were exposed to the virus at a young age, delaying first exposure to older age groups. This shift resulted in more severe outbreaks among adolescents and adults, who were more likely to develop paralytic polio. Paradoxically, better hygiene created conditions for more visible and alarming epidemics, even as overall incidence was declining.
Economic and behavioral changes also contributed to the pre-vaccine decline. Urbanization brought families into closer living quarters, increasing virus transmission but also fostering herd immunity as more individuals were exposed and recovered. Additionally, public health campaigns in the mid-20th century emphasized quarantine measures, such as closing public pools and limiting social gatherings during outbreaks, which temporarily reduced spread. These measures, combined with improved nutrition and general health, likely played a role in lowering polio rates before vaccines became available.
Comparatively, the decline in polio incidence before vaccination highlights the interplay between environmental, social, and biological factors in disease control. While vaccines ultimately eradicated polio in many regions, the pre-vaccine decline demonstrates that public health interventions can significantly alter disease trajectories. This historical context underscores the importance of multifaceted approaches to infectious disease management, blending sanitation, education, and medical innovation. Understanding these dynamics offers valuable lessons for addressing contemporary health challenges, where environmental and behavioral factors often intersect with medical solutions.
Does Truist Bank Offer a Christmas Club Savings Account?
You may want to see also
Explore related products






![]()
Improved sanitation impact on polio
The decline of polio in the early 20th century cannot be discussed without acknowledging the pivotal role of improved sanitation. Before the vaccine, public health measures, particularly in wastewater management and clean water access, significantly reduced the virus's transmission. In cities like New York, the installation of comprehensive sewer systems in the 1920s and 1930s coincided with a sharp drop in polio cases. This wasn’t mere coincidence; it was a direct result of breaking the fecal-oral transmission chain, the primary route of poliovirus spread.
Consider the mechanics: poliovirus thrives in contaminated water and food. By ensuring that human waste was no longer a part of the water supply, sanitation improvements effectively starved the virus of its transmission pathways. For instance, in rural areas where outhouses replaced open defecation, polio incidence decreased by as much as 40% within a decade. This wasn’t just about infrastructure—it was about behavioral change. Communities that adopted boiling water before consumption or using chlorine tablets saw even greater declines, demonstrating that sanitation is both a structural and a personal responsibility.
However, sanitation alone wasn’t a silver bullet. While it drastically reduced sporadic cases, it couldn’t eliminate the virus entirely. Poliovirus is highly contagious, and even in sanitized environments, close contact could still lead to outbreaks. For example, despite improved sanitation, summer polio epidemics persisted in the U.S. until the 1950s, particularly in crowded urban areas where the virus could still find pockets of transmission. This highlights the limitations of sanitation: it controls spread but doesn’t confer immunity.
To replicate the success of sanitation measures today in low-resource settings, focus on three key steps: first, invest in community-level wastewater treatment systems, even if they’re low-tech. Second, educate populations on handwashing with soap, especially after using the toilet and before handling food. Third, monitor water quality regularly, using simple test kits to detect contamination. Pair these with vaccination campaigns, as sanitation and immunization are complementary, not competing strategies. The lesson from history is clear: sanitation laid the groundwork, but the vaccine delivered the knockout punch.
Securing Banking Networks: Strategies for Effective Network Segregation
You may want to see also
Explore related products






![]()
Historical polio incidence trends
Polio incidence rates in the early 20th century exhibited a cyclical pattern, with periodic outbreaks occurring every few years. These epidemics were particularly severe in industrialized nations, where improved sanitation paradoxically contributed to a loss of natural immunity in the population. For instance, in the United States, major outbreaks in the 1940s and 1950s led to thousands of cases annually, with children under five being the most vulnerable. This trend highlights the virus's ability to thrive in environments where it had not been previously widespread, a phenomenon known as the hygiene hypothesis.
Analyzing historical data reveals that polio incidence was not uniformly distributed across regions or socioeconomic groups. Urban areas, with their higher population densities, often experienced more significant outbreaks compared to rural communities. Additionally, lower socioeconomic status was correlated with increased risk, likely due to poorer living conditions and limited access to healthcare. For example, in the 1916 New York City epidemic, tenement districts reported significantly higher case rates than more affluent neighborhoods. This disparity underscores the role of environmental factors in disease transmission.
Efforts to control polio before the vaccine focused on quarantine measures, improved sanitation, and public health campaigns. During outbreaks, public swimming pools were often closed, and children were advised to avoid crowded places. While these measures helped reduce transmission temporarily, they did not prevent the cyclical return of the disease. For instance, the use of iron lungs to support paralyzed patients became a symbol of the era, but such interventions were reactive rather than preventive. This reliance on symptomatic treatment and containment strategies limited the long-term impact on incidence rates.
Comparing polio trends across countries provides further insight into pre-vaccine management. In Scandinavian nations, where public health infrastructure was robust, incidence rates were lower and outbreaks less severe than in other parts of Europe. These countries implemented systematic surveillance and isolation protocols, demonstrating that organized public health efforts could mitigate, though not eliminate, the disease. However, even in these regions, polio remained a persistent threat until the introduction of the vaccine.
The historical incidence trends of polio illustrate the limitations of pre-vaccine interventions. While public health measures could temporarily suppress outbreaks, they failed to eradicate the disease or confer lasting immunity. The cyclical nature of epidemics, combined with the virus's ability to exploit susceptible populations, ensured that polio remained a significant global health challenge. This context is crucial for understanding why the development of the polio vaccine in the 1950s marked a turning point, shifting the focus from containment to prevention and ultimately leading to the near-eradication of the disease.
Efficient Banking Operations: Managing Transactions Across Three Servers
You may want to see also
Explore related products






![]()
Role of hygiene in polio reduction
Polio cases plummeted in many developed nations before the vaccine's arrival, and improved hygiene played a starring role in this decline. This wasn't a simple coincidence. The poliovirus thrives in environments with poor sanitation, where fecal-oral transmission is common. Think contaminated water sources, inadequate sewage systems, and crowded living conditions.
The Hygiene Arsenal:
Imagine a multi-pronged attack on the poliovirus. Clean water, a cornerstone of hygiene, became increasingly accessible through filtration systems and chlorination. This single measure drastically reduced the virus's ability to spread through drinking water. Sanitation systems evolved, separating human waste from living areas and preventing its re-entry into the environment. Personal hygiene practices, like handwashing with soap, became more widespread, breaking the chain of infection at a crucial point.
Think of it like this: hygiene acted as a firewall, preventing the poliovirus from finding new hosts and establishing a foothold in communities.
Beyond the Obvious: Hygiene's impact went beyond just preventing direct transmission. Improved living conditions, often a byproduct of better hygiene, meant less overcrowding. This reduced the likelihood of close contact between infected and susceptible individuals, further slowing the virus's spread. Additionally, better nutrition, often linked to improved hygiene, strengthened immune systems, making individuals less susceptible to severe polio infections.
It's important to note that hygiene alone didn't eradicate polio. The vaccine was the decisive blow. However, hygiene laid the groundwork, creating an environment where the vaccine could be most effective.
Lessons for Today: The polio story offers valuable lessons for tackling other infectious diseases. Investing in basic hygiene infrastructure – clean water, sanitation, and education on handwashing – remains a powerful tool in our arsenal. These measures not only combat specific diseases but also contribute to overall public health and well-being. The fight against polio reminds us that sometimes, the most effective solutions are the simplest ones.
Safely Remove Bank Details from Tombola: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Polio surveillance before vaccination era
Before the advent of the polio vaccine, surveillance efforts were the cornerstone of understanding and managing the disease. These initiatives, though rudimentary by today’s standards, laid the groundwork for global eradication strategies. Public health officials relied on passive reporting systems, where physicians voluntarily notified local health departments of suspected cases. This method, while imperfect, provided critical insights into polio’s geographic spread and seasonal patterns. For instance, in the United States during the 1940s and 1950s, surveillance data revealed that polio cases peaked in the summer months, a trend that guided public health interventions like pool closures and quarantine measures.
One of the most significant challenges in pre-vaccine polio surveillance was the lack of standardized diagnostic tools. Diagnosis often depended on clinical symptoms, such as limb paralysis or muscle weakness, which could mimic other conditions like Guillain-Barré syndrome. Laboratory confirmation was limited to detecting the virus in stool samples or cerebrospinal fluid, a process that was time-consuming and inaccessible in many regions. Despite these limitations, surveillance efforts identified high-risk groups, such as children under five, who accounted for approximately 50% of reported cases. This knowledge informed targeted prevention strategies, including isolating infected individuals and educating parents on hygiene practices.
The global nature of polio demanded international collaboration in surveillance, yet this was rarely achieved before the vaccine era. Wealthier nations like the United States and the United Kingdom maintained more robust systems, while many low-income countries lacked the infrastructure to track cases effectively. The World Health Organization (WHO), established in 1948, began to coordinate efforts, but its impact was limited by resource constraints. For example, in India, surveillance was sporadic, with many cases going unreported due to poor healthcare access. This disparity highlights the uneven progress in understanding polio’s true burden before vaccination.
A critical takeaway from pre-vaccine surveillance is its role in dispelling myths about polio’s inevitability. Data collected during this era demonstrated that the disease was not uniformly fatal or disabling; approximately 72% of infections were asymptomatic, and only 1% resulted in permanent paralysis. This knowledge shifted public perception from fear to actionable awareness. Moreover, surveillance identified environmental factors, such as overcrowding and poor sanitation, as contributors to outbreaks. These insights, though incomplete, paved the way for the vaccine’s development and the eventual eradication efforts that followed.
In retrospect, polio surveillance before the vaccine era was a testament to human ingenuity in the face of limited technology. It underscored the importance of data collection, even when tools were imperfect, and highlighted the need for global cooperation. While the vaccine ultimately became the game-changer, surveillance efforts provided the foundation for understanding polio’s behavior, enabling public health officials to act strategically rather than reactively. This historical context remains relevant today, offering lessons for combating emerging infectious diseases.
Understanding DDR: Decoding Its Meaning and Role in Banking Operations
You may want to see also
Frequently asked questions
No, polio was not almost eradicated before the vaccine. In fact, polio cases were widespread and increasing in many parts of the world before the introduction of the polio vaccine in the 1950s.
While improved sanitation and hygiene helped reduce the transmission of some diseases, they did not significantly decrease polio cases. Polio remained a major public health threat until the vaccine was introduced.
There were no effective treatments or cures for polio before the vaccine. Medical interventions, such as the iron lung, only provided temporary support for breathing in severe cases but did not eradicate the disease.
No, polio did not naturally decline before the vaccine. In fact, polio outbreaks were increasing in frequency and severity in the early 20th century, particularly in developed countries, until the vaccine became widely available.