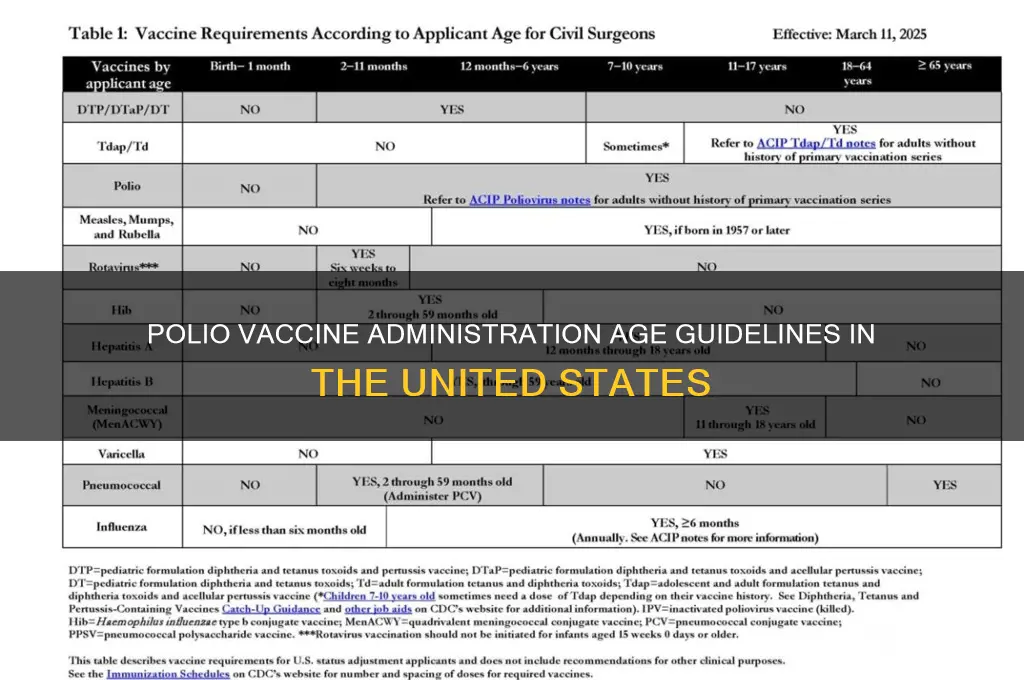
In the United States, the polio vaccine is typically administered as part of the routine childhood immunization schedule to ensure protection against poliomyelitis, a highly contagious and potentially paralyzing disease. The Centers for Disease Control and Prevention (CDC) recommends that children receive a series of four doses of the inactivated poliovirus vaccine (IPV), starting at 2 months of age, followed by additional doses at 4 months, 6-18 months, and 4-6 years. This schedule is designed to provide robust immunity during early childhood, when the risk of exposure and severe complications is highest. While polio has been eradicated in the U.S. since 1979, vaccination remains crucial to prevent reintroduction of the virus from other parts of the world. Adults who are at increased risk, such as travelers to polio-endemic regions or healthcare workers, may also require vaccination or booster doses, as determined by their healthcare provider.
| Characteristics | Values |
|---|---|
| Recommended Age for First Dose | 2 months |
| Subsequent Doses | 4 months, 6-18 months, and 4-6 years |
| Total Number of Doses | 4 doses |
| Vaccine Type | Inactivated Poliovirus Vaccine (IPV) |
| Administration Route | Intramuscular or subcutaneous injection |
| Purpose | Protection against poliomyelitis (polio) |
| Vaccine Brand Examples (USA) | Ipol (Sanofi Pasteur), Pediarix (combination vaccine, GSK) |
| Catch-up Vaccination | Unvaccinated children and adults can receive catch-up doses |
| Booster Dose for Adults | Not routinely recommended, but may be advised for specific risk groups |
| Vaccine Effectiveness | Over 99% effective after 3 doses |
| Side Effects | Mild, including soreness at injection site, fever, irritability |
| Contraindications | Severe allergic reaction to a previous dose or vaccine component |
| CDC and AAP Recommendations | Follow the recommended immunization schedule |
| Global Eradication Status | Polio is nearly eradicated globally, but vaccination remains crucial |
Explore related products






What You'll Learn
![]()
Recommended Polio Vaccine Schedule
In the United States, the polio vaccine is administered following a specific schedule designed to provide robust immunity during critical developmental stages. The Centers for Disease Control and Prevention (CDC) recommends a series of four doses, starting at 2 months of age. This initial dose is followed by subsequent shots at 4 months, 6–18 months, and 4–6 years. This staggered approach ensures that children build and maintain strong immunity against poliovirus, a once-devastating disease now nearly eradicated globally due to widespread vaccination efforts.
The first three doses of the polio vaccine, typically administered as part of the inactivated poliovirus vaccine (IPV), are crucial for establishing a foundation of immunity. Each dose contains 0.5 mL and is given via intramuscular or subcutaneous injection. The timing of these doses is deliberate: the 2-month shot primes the immune system, the 4-month dose boosts the response, and the 6–18-month dose solidifies protection. Parents should ensure their child receives these doses on schedule, as delays can leave them vulnerable during periods of higher exposure risk, such as when entering daycare or preschool.
The final dose, given between 4–6 years of age, serves as a critical reinforcement of immunity. This booster is often administered just before children enter elementary school, a setting where close contact increases the risk of disease transmission. While this dose is the last in the standard series, it’s not optional—it ensures long-term protection into adulthood. For children who missed earlier doses, healthcare providers may adjust the schedule to catch them up, but the goal remains the same: completing the full series for maximum protection.
Practical tips for parents include scheduling vaccinations during well-child visits to minimize stress and ensuring the child’s immunization record is up to date. Mild side effects, such as soreness at the injection site, are common but short-lived. Rarely, fever or fussiness may occur, but these are far outweighed by the vaccine’s benefits. For families traveling to regions where polio remains endemic, confirming full vaccination status is essential, as the disease can still pose a threat in certain parts of the world.
Comparatively, the U.S. schedule aligns with global recommendations but differs slightly from countries using oral polio vaccine (OPV), which is more common in regions actively combating polio outbreaks. The U.S. exclusively uses IPV due to its safety profile and effectiveness. While OPV provides intestinal immunity and can stop person-to-person spread, it carries a minuscule risk of vaccine-derived poliovirus, making IPV the preferred choice in polio-free countries like the U.S. This tailored approach reflects the nation’s success in eliminating the disease while maintaining vigilance through vaccination.
From Ledgers to Computers: The Evolution of Banking Record-Keeping
You may want to see also
Explore related products






![]()
Infant Polio Vaccination Timing
In the United States, the polio vaccine is administered to infants as part of a carefully timed series to ensure robust immunity. The Centers for Disease Control and Prevention (CDC) recommends a four-dose schedule, starting at 2 months of age, followed by doses at 4 months, 6 through 18 months, and a final booster at 4 through 6 years. This staggered approach allows the immune system to build and maintain protection against poliovirus effectively. Each dose is critical, as skipping or delaying shots can leave a child vulnerable during periods of heightened susceptibility.
The timing of these doses is not arbitrary but rooted in immunological science. At 2 months, an infant’s immune system is mature enough to respond to the vaccine, yet young enough to begin building immunity early. The 4-month dose reinforces this initial response, while the 6 through 18-month dose ensures long-term immunity is established. The final booster at 4 through 6 years coincides with school entry, providing an additional layer of protection during a time when children are more likely to encounter pathogens. This schedule balances the need for early protection with the immune system’s developmental milestones.
Practical considerations for parents include ensuring timely appointments and understanding potential side effects, which are typically mild (e.g., soreness at the injection site or low-grade fever). It’s crucial to adhere to the recommended timeline, as delays can disrupt the immune response. For example, if the second dose is significantly postponed, the interval between doses may need adjustment to maintain efficacy. Parents should also be aware that the polio vaccine is often administered as part of a combination vaccine (e.g., DTaP-IPV-Hib), simplifying the immunization process and reducing the number of injections required.
Comparatively, this schedule contrasts with those in some other countries, where a three-dose series may be used. However, the U.S.’s four-dose approach is designed to account for the specific strains of poliovirus and the population’s immune response patterns. This tailored strategy reflects the ongoing vigilance against polio, a disease once feared globally but now nearly eradicated due to widespread vaccination efforts. By following this timeline, parents play a vital role in safeguarding their children and contributing to public health.
In conclusion, the infant polio vaccination timing in the U.S. is a meticulously designed process that prioritizes both individual and community immunity. Adhering to the 2, 4, 6-18 months, and 4-6 years schedule ensures children are protected during critical developmental stages. Parents should view this timeline not as a suggestion but as a cornerstone of their child’s health, backed by decades of scientific research and public health success. Timely vaccination is a simple yet powerful act that preserves the progress made against polio and prevents its resurgence.
Mastering the Federal Bank Clerk Exam: Proven Strategies for Success
You may want to see also
Explore related products






![]()
Booster Doses for Polio
In the United States, the polio vaccine is typically administered in a series of doses during childhood, starting at 2 months of age. However, the conversation around booster doses for polio is crucial, especially for maintaining long-term immunity and preventing potential outbreaks. Booster doses are not routinely required for the general population but are recommended in specific scenarios, such as travel to polio-endemic regions or for individuals at higher risk of exposure.
From an analytical perspective, the Centers for Disease Control and Prevention (CDC) guidelines emphasize that the initial polio vaccine series provides robust protection. The standard schedule includes four doses: at 2 months, 4 months, 6–18 months, and 4–6 years of age. This regimen ensures that over 99% of recipients develop immunity. However, immunity can wane over time, particularly in individuals who received the inactivated polio vaccine (IPV) rather than the oral polio vaccine (OPV), which was phased out in the U.S. due to rare cases of vaccine-derived polio. For adults traveling to areas with active polio transmission, a one-time booster dose of IPV is recommended if it has been 10 or more years since their last dose.
Instructively, administering a polio booster is straightforward. The IPV booster dose is the same as the primary doses—0.5 mL for children and adults. Healthcare providers should review an individual’s vaccination history to determine eligibility. For example, if a traveler received their last polio dose as a child, a single booster is sufficient to restore protection. It’s important to schedule the booster at least 4–8 weeks before travel to ensure immunity is established. Practical tips include carrying proof of vaccination, as some countries require it for entry, and consulting a healthcare provider or travel clinic for personalized advice.
Comparatively, the approach to polio boosters in the U.S. differs from global strategies. In polio-endemic countries, frequent campaigns administer oral polio vaccine boosters to all children under 5, regardless of prior vaccination status. This method aims to interrupt virus transmission in communities. In contrast, the U.S. focuses on individual risk assessment, reserving boosters for specific groups like travelers, healthcare workers, or laboratory personnel handling poliovirus. This targeted approach reflects the country’s polio-free status since 1979 and the low risk of domestic transmission.
Persuasively, ensuring up-to-date polio vaccination, including boosters when necessary, is a critical public health measure. While polio has been nearly eradicated globally, recent detections of vaccine-derived poliovirus in New York and London serve as reminders that the disease can reemerge in underimmunized populations. Booster doses not only protect individuals but also contribute to herd immunity, safeguarding those who cannot be vaccinated due to medical reasons. By staying informed and adhering to CDC recommendations, individuals play a vital role in preventing the resurgence of this once-devastating disease.
How to Buy Lloyds Bank Shares: A Step-by-Step Guide
You may want to see also
Explore related products






![]()
Polio Vaccine Age Limits
In the United States, the polio vaccine is typically administered in a series of doses starting at 2 months of age, with subsequent doses given at 4 months and 6 through 18 months. This schedule, recommended by the Centers for Disease Control and Prevention (CDC), ensures robust immunity during early childhood when vulnerability to polio is highest. The vaccine, available in both inactivated (IPV) and oral (OPV) forms, is exclusively administered as IPV in the U.S. due to its safety profile and effectiveness. While the primary series concludes by age 2, a booster dose is recommended between 4 and 6 years to reinforce long-term protection. This structured approach reflects decades of public health success, nearly eradicating polio domestically.
The age limits for polio vaccination are not arbitrary but are rooted in immunological science and disease epidemiology. Infants under 2 months are excluded from the initial dose due to the immature immune response, while delaying the series beyond 6 months increases exposure risk during critical developmental stages. For adults, the CDC advises vaccination only in specific scenarios: unvaccinated individuals traveling to polio-endemic regions or healthcare workers handling poliovirus materials. Notably, adults receive a 3-dose series with intervals of 4 to 8 weeks between the first and second doses, and 6 to 12 months before the third. This tailored approach balances immunity needs with the rarity of polio in the U.S., where the last case of wild poliovirus occurred in 1979.
A comparative analysis highlights the contrast between U.S. and global polio vaccination strategies. In endemic countries, the oral polio vaccine (OPV) remains prevalent due to its ease of administration and ability to induce intestinal immunity, curbing viral transmission. However, the U.S. exclusively uses IPV to eliminate the rare risk of vaccine-derived poliovirus (VDPV) associated with OPV. This divergence underscores the adaptability of vaccination programs to regional disease burdens and healthcare infrastructure. For travelers from the U.S. to high-risk areas, the CDC mandates proof of vaccination or a single-dose booster for adults previously vaccinated as children, ensuring global health security without compromising domestic safety.
Practical considerations for parents and caregivers include adhering strictly to the CDC schedule, as delays can leave children susceptible during outbreaks. Schools and childcare facilities often require proof of vaccination, making timely completion essential. For adults seeking vaccination, consulting a healthcare provider is critical to assess risk factors and determine eligibility. Notably, pregnancy is not a contraindication for IPV, offering protection to both mother and fetus. Cost should not be a barrier, as the Vaccines for Children (VFC) program covers eligible children, while most insurance plans include adult vaccines. This combination of accessibility and medical precision exemplifies the polio vaccine’s role as a cornerstone of preventive healthcare.
Jessica Raine's Role in Saving Mr. Banks: Fact or Fiction?
You may want to see also
Explore related products






![]()
Catch-Up Vaccination Guidelines
In the United States, the polio vaccine is typically administered as part of the routine childhood immunization schedule, starting at 2 months of age. However, life happens—appointments are missed, records are lost, or families relocate. For those who fall behind, catch-up vaccination guidelines ensure that individuals can still achieve immunity against polio. These guidelines are structured to accommodate different age groups and vaccination histories, providing a clear pathway to protection.
For children who start the polio vaccine series late, the Centers for Disease Control and Prevention (CDC) recommends a flexible approach. If the first dose is given after the recommended 2-month mark, the subsequent doses should be administered 4–8 weeks apart, with a minimum interval of 4 weeks between doses. For example, a child who begins the series at 6 months would receive doses at 6, 10, and 14 months, followed by a booster at 4–6 years. This ensures the immune system has adequate time to build a robust response without overloading it.
Adolescents and adults who have never been vaccinated or have incomplete records face a different set of guidelines. The CDC advises a 3-dose series for those aged 7–18 years, with doses spaced 4–8 weeks apart, followed by a booster 6–12 months after the third dose. Adults require a similar 3-dose series, but the urgency increases if they are traveling to areas where polio is still endemic. In such cases, accelerating the schedule—administering doses at 0, 1–2 months, and 6–12 months—can provide quicker protection, though this may require careful monitoring for potential side effects.
Practical tips can make catch-up vaccination smoother. Always bring any available vaccination records to the appointment, even if incomplete, as healthcare providers can use them to determine the best course of action. For families with limited access to healthcare, public health clinics and school-based programs often offer catch-up vaccinations at reduced or no cost. Additionally, setting reminders for follow-up doses can prevent further delays and ensure the series is completed as recommended.
Blood Bank Storage: Safeguarding Life-Saving Donations for Transfusions
You may want to see also
Frequently asked questions
The first dose of the polio vaccine (IPV) is typically administered at 2 months of age as part of the routine childhood immunization schedule in the USA.
Children in the USA receive a total of 4 doses of the polio vaccine (IPV). The doses are administered at 2 months, 4 months, 6-18 months, and 4-6 years of age.
Yes, the polio vaccine is mandatory for school entry in the USA. Most states require children to have completed at least 3 doses of the polio vaccine by kindergarten entry (around 4-6 years of age), with the final dose given after 4 years of age.